
- Medically Reviewed by: Mr Mfazo Hove, Consultant Ophthalmic Surgeon
- Author: Mr Mfazo Hove
- Published: June 16, 2026
- Last Updated: June 18, 2026
The Most Important Part of Cataract Surgery Happens Before Surgery
Cataract surgery is no longer just cataract surgery. It is refractive surgery. Patients who walk into a private ophthalmology clinic in 2026 are not asking whether they will see better. They are asking whether they will see well enough to drive without glasses, read a phone in low light, work at a screen all day, and not feel the gradient between near and distance work that defines a multifocal life.
The conversation that follows, about premium intraocular lenses, target refraction and spectacle independence, is shaped almost entirely by what the patient expects of the result. And yet most of that conversation, in most clinics, happens before anyone has properly measured the eye.
Most public commentary about cataract surgery centres on the lens, the laser, or the surgeon. Almost no one discusses the quality of the measurements used to plan the surgery in the first place. This is the silent foundation on which every refractive outcome rests⁶. When measurements are accurate, lens calculations are accurate. When lens calculations are accurate, refractive surprises are rare. When measurements are wrong, even by small amounts, no surgical technique can rescue the result.
At Blue Fin Vision®, we have built our preoperative workup around a deliberately overspecified principle: every cataract and lens replacement patient receives biometry on two independent platforms, using two different physical technologies, and the two outputs must agree before a refractive plan is finalised. We call this double biometry, and it is performed routinely on every patient, not as a salvage workflow for difficult cases, but as the default.
In modern cataract surgery, precision is not luck. It is the result of systems deliberately designed to reduce uncertainty.
What Is Biometry?
Biometry is the set of optical measurements taken before cataract or lens replacement surgery that determine which intraocular lens (IOL) is implanted, at what power, and with what target refraction. The key measurements are:
- Axial length, the distance from the front of the cornea to the retina, typically 22 to 25 mm in an average eye. This is the single most powerful determinant of IOL power.
- Corneal curvature, expressed as K-values or K-means, the refractive contribution of the cornea, the eye’s most powerful lens.
- Anterior chamber depth (ACD), the distance from the cornea to the front surface of the natural lens. This is used to predict where the implanted IOL will sit.
- Lens thickness, the dimension of the patient’s own crystalline lens, increasingly used in modern formulae.
- Central corneal thickness (CCT), relevant to corneal health, glaucoma monitoring, and refractive planning.
- White-to-white corneal diameter, used in some toric and phakic IOL calculations.
These measurements feed into a modern IOL calculation formula (Barrett Universal II, Haigis, Hill-RBF, Hoffer Q, or one of several newer alternatives⁷) and the formula returns the implant power that should leave the patient closest to the agreed target refraction. Modern cataract surgery is essentially a precision engineering exercise measured in fractions of a millimetre.
A 0.10 mm error in axial length translates to roughly 0.27 D of refractive error in an average eye. A 0.25 D error in K-mean translates to roughly 0.25 D of refractive error. Stack these errors and the patient who was meant to be plano sits at -0.75 D and needs distance correction for the rest of their life. This is the unforgiving arithmetic of refractive surgery.

Why Most Clinics Use Only One Biometry Machine
The standard preoperative workflow in most cataract clinics, NHS and private alike, is single-device biometry. The patient is scanned on a single optical biometer, usually an IOLMaster 500/700 or a Lenstar LS900. If the scan is poor quality, it is repeated on the same machine. If the device fails to acquire an axial length (which still happens in dense cataracts), the patient is referred for ultrasound biometry as a backup.
Read more on what happens when the cataract is too dense for optical biometry.
This workflow is not wrong. It is the result of operational pressure: clinic footprint, equipment cost, training overheads, time per patient, and the perfectly reasonable assumption that a single high-quality optical biometer is usually enough. For the majority of patients receiving a standard monofocal IOL aimed at plano with spectacles for reading, it is enough.
But the same workflow is also why second measurements are conventionally reserved for “problem cases”, extreme axial lengths, prior refractive surgery, dense posterior subcapsular cataracts, or patients where the surgeon already suspects a refractive surprise risk. The second device is treated as a diagnostic tool, not a quality control tool.
In many clinics, second measurements are reserved for problem cases. At Blue Fin Vision®, they are standard for everyone.
The distinction matters. A second measurement performed only when the first one looks wrong selects only the cases where the surgeon already had doubt. A second measurement performed on every patient catches the cases where the surgeon had no doubt, and should have done.
The Blue Fin Vision® Approach: Double Biometry for Every Patient
Every patient assessed for cataract surgery or refractive lens exchange at Blue Fin Vision® undergoes biometry on two independent platforms during the same preoperative visit:
- Lenstar LS900 (Haag-Streit), optical low-coherence reflectometry. This is the platform whose output feeds directly into the IOL calculation.
- REVO FC (Optopol), spectral-domain OCT biometry (B-OCT) combined with anterior segment OCT and full corneal topography.
The two devices use fundamentally different physical principles to measure the same eye. Lenstar uses an 820 nm super-luminescent diode to make optical distance measurements between the corneal apex, lens surfaces and retina. REVO FC uses spectral-domain OCT to image those same structures and derives axial length from the imaged geometry directly. Inter-device agreement studies, including direct head-to-head comparisons of the REVO and Lenstar platforms, have repeatedly shown that these technologies agree to within 0.01 to 0.02 mm of axial length on average across normal cataract populations¹ ² ³ ⁴ ⁵ ⁹.
Figure A: The Two Pathways, Side by Side
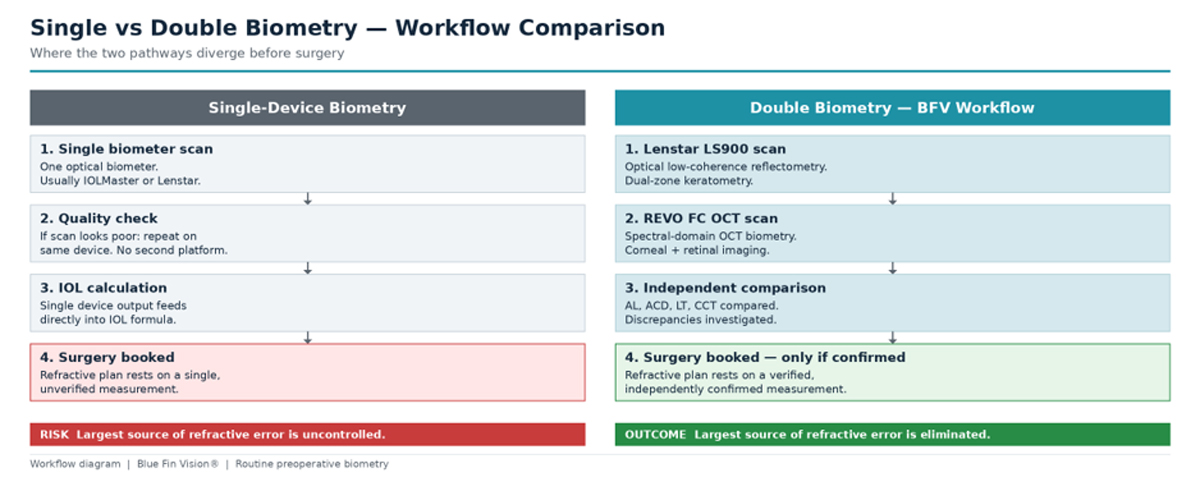
Single vs Double Biometry workflow comparison. The pathways are identical until the moment of independent confirmation, and that moment is where preventable refractive error is controlled.
What we are doing is not redundancy. It is independent confirmation. If both platforms agree, the lens calculation rests on the firmest possible foundation. If they disagree, even by clinically small amounts, the disagreement is the signal. We re-scan, investigate the cause, and resolve it before surgery is booked.
The clinical objective is not simply to measure twice. It is to obtain two independently derived answers to the same question, then refuse to proceed with surgery until those answers agree.
Why We Use Two Different Technologies
Lenstar LS900

The Lenstar LS900 has been one of the most widely validated optical biometers in clinical use since its introduction. Reproducibility studies have reported coefficients of variability under 0.9% across all measured parameters⁴, and direct agreement studies against the IOLMaster have shown that axial length and IOL power calculated from Lenstar are biometrically equivalent to those derived from partial coherence interferometry³ ⁵. The Lenstar feeds its measurements into a built-in EyeSuite calculator that returns implant powers across multiple formulae (Haigis, Barrett Universal II, Hill-RBF, SRK/T and Hoffer Q) in a single workflow.
REVO FC OCT

The REVO FC is a spectral-domain OCT platform that performs axial length biometry, full corneal topography, anterior segment OCT and posterior segment OCT in a single device. Its B-OCT axial length measurement has been validated against the swept-source IOLMaster 700 with intraclass correlation coefficients of 1.000 for axial length in both healthy and cataractous eyes and mean axial length differences in the order of 0.001 mm¹. Crucially, B-OCT also provides visual confirmation: the operator can see the OCT trace and the structural landmarks the device has used to derive each measurement, which is impossible on optical biometry alone.
Read more about what an OCT scan is.
Why This Matters
The two platforms are not duplicate machines. Lenstar provides the IOL power calculation. REVO FC provides the surrounding evidence: tomographic confirmation of axial length, anterior and posterior corneal topography, the pachymetric map, and the real (total) corneal power that no two-surface keratometer can produce.
Lenstar tells us what lens to implant. REVO FC tells us whether we should trust that answer.
Real-World Example: Double Biometry in Practice
The clinical value of double biometry only becomes visible when two independently engineered platforms, one optical and one OCT-based, are placed side by side and asked the same question. The following case demonstrates what we look for, and what we have come to expect.
All identifiers have been removed. The measurements shown are the actual scan outputs from a routine pre-operative workup for cataract or refractive lens exchange surgery.
Figure 1: Inter-Device Agreement, Both Eyes
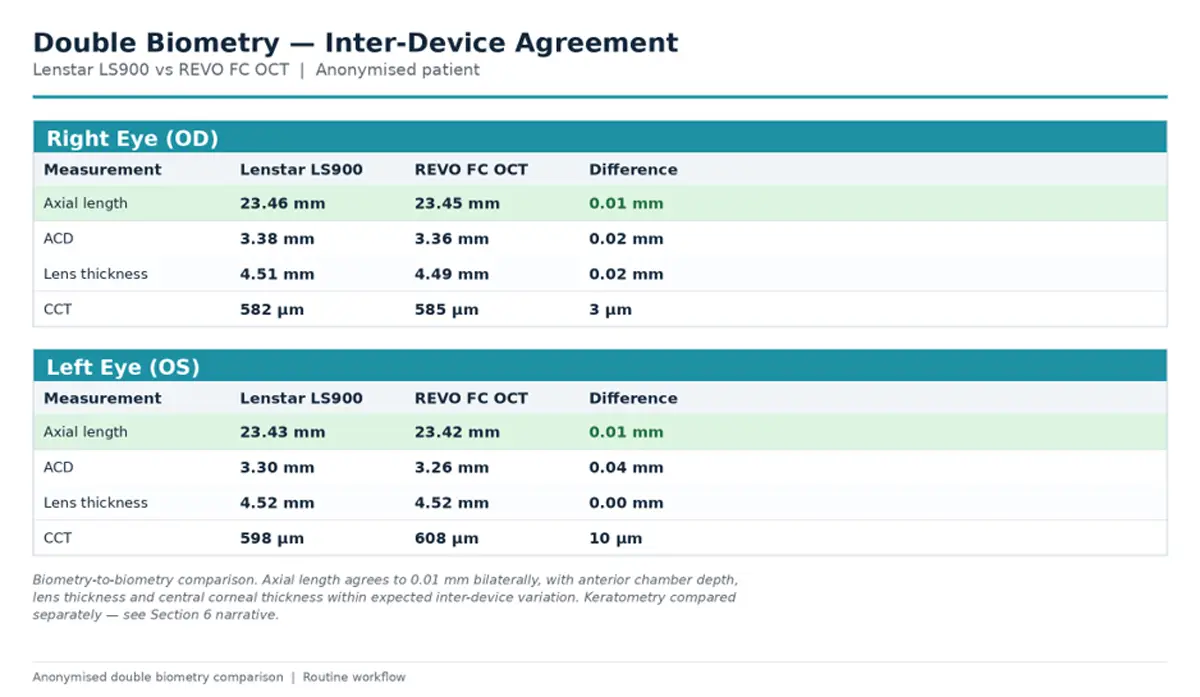
Lenstar LS900 (optical biometry) and REVO FC (OCT biometry) compared across the principal pre-operative measurements. Axial length agreement bilaterally highlighted in green.
Right Eye
Axial length on Lenstar LS900 was 23.46 mm. The REVO FC OCT biometer, averaging ten independent scans, returned 23.45 mm. The two devices, working from entirely different physical principles, agreed to one hundredth of a millimetre.
Anterior chamber depth differed by 0.02 mm. Lens thickness differed by 0.02 mm. Central corneal pachymetry differed by 3 µm. These are the parameters that feed directly into the IOL power calculation, and the inter-device agreement is what we expect from two well-engineered, well-calibrated platforms.
Left Eye
Axial length on Lenstar LS900 was 23.43 mm. REVO FC OCT returned 23.42 mm. Again, agreement to 0.01 mm. Lens thickness was identical at 4.52 mm. Anterior chamber depth differed by 0.04 mm. Central corneal pachymetry differed by 10 µm, the largest single difference in the dataset, but well within the published 95% limits of agreement between optical low-coherence reflectometry and OCT-based CCT.
Keratometry: A Clinical Decision, Not a Comparison
Keratometry is deliberately absent from the comparison table above, and the reason is visible on the topography scans themselves. Both eyes show partial upper eyelid coverage of the superior cornea on the REVO topography acquisitions, and the device has flagged the scans accordingly with a topography quality (TQF) warning. This is a common feature of routine topography in patients with normal lid anatomy: the upper lid sits over the superior cornea, and ring acquisition in the affected sector becomes incomplete.
In this situation, the K-values derived from a TQF-flagged topography acquisition are not a like-for-like comparator for the dual-zone keratometry produced by the Lenstar LS900, which uses a 32-point ring measurement specifically designed for IOL power calculation. The two measurements are answering related but not identical questions over different parts of the cornea. Comparing them directly would generate a number, and that number would be clinically meaningless.
Our internal rule is straightforward and consistently applied: where REVO topography and Lenstar keratometry diverge in the presence of an acquisition artefact, the Lenstar value is used for the IOL power calculation. The REVO topography is then interpreted qualitatively for what it does uniquely well: overall corneal shape, posterior elevation, pachymetric distribution, and the regularity of the astigmatic pattern across the entire imaged area. That is exactly the role each device is engineered for.
The goal is not merely to measure the eye twice. The goal is to independently confirm the same refractive plan using two different technologies.
Figure 2: REVO FC Anterior Topography, Right Eye
The REVO FC scan provides clinical information that no biometer alone can deliver: anterior and posterior corneal elevation, full pachymetric map, real (total) corneal power, and a tangential curvature display. These maps are what tell us whether a premium IOL is safe to recommend, and whether the K-values entering the lens calculation can be trusted.
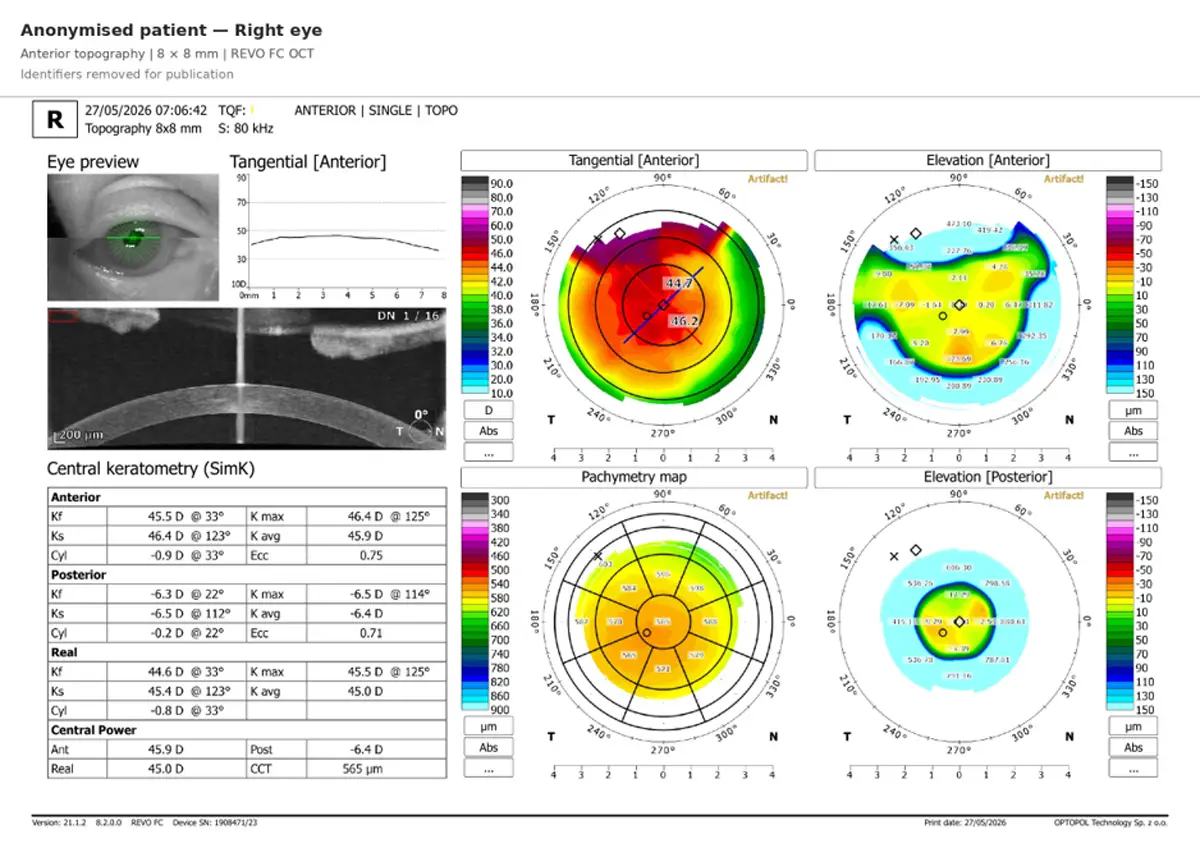
Anonymised REVO FC anterior topography, 8 × 8 mm scan. Partial upper eyelid coverage of the superior cornea is visible as the dark sector on the tangential map and is responsible for the topography quality (TQF) warning. Posterior elevation and pachymetric maps confirm a healthy cornea suitable for refractive lens surgery.
Why This Case Is Unremarkable, and Why That Is the Point
There is nothing surgically unusual about this patient. That is the entire argument. When the two biometers agree to 0.01 mm of axial length bilaterally, the lens power calculation rests on the firmest possible foundation. The conversation with the patient about target refraction, IOL choice and realistic expectations can be conducted with confidence rather than hedged language.
When they disagree, even by small amounts that would be invisible on a single-device workup, we re-scan, investigate the cause, and resolve it before surgery is booked. That is the operational meaning of performing double biometry routinely rather than reactively.
A refractive surprise is rarely the fault of the surgery. It is almost always the fault of the measurement that preceded it.
What if the Two Devices Disagree?
Inter-device agreement is the goal. Disagreement is the signal. When the Lenstar and the REVO FC produce different values for axial length, anterior chamber depth, lens thickness, or central corneal thickness, beyond the small inter-device variation expected from two well-calibrated platforms, the Blue Fin Vision® workflow does not proceed.
Blue Fin Vision® Protocol: Inter-Device Disagreement
- Step 1. Re-scan on both platforms in the same visit. Many small discrepancies resolve immediately and reflect a single suboptimal acquisition rather than a real inter-device difference.
- Step 2. Investigate the cause. Common contributors include unstable tear film, fixation drift, partial lid coverage on one platform, eye movement during acquisition, or dense lens opacity at one specific scanning wavelength.
- Step 3. Resolve before booking. If a clinically relevant disagreement persists after re-scanning, the patient is re-appointed for further investigation, never proceeded to surgery with an unresolved measurement discrepancy.
- Step 4. Document the decision. Every resolution is recorded in the clinical record alongside the final biometric values used for the IOL calculation.
This protocol is what gives the underlying claim, “double biometry catches what single biometry cannot”, its operational meaning. The workflow does not just produce more measurements. It produces a defined response to disagreement.
Why This Matters to Patients
Patients almost never see their biometry workup. They sit in a chair, rest their chin on a pad, look at a fixation target, and the scan is over in under a minute. Whatever is happening behind the screen happens out of sight. The result reaches them in the consultation room as a recommended lens power and a target refraction.
But the consequences of that invisible workup are not invisible. They show up six weeks after surgery, when the patient either reads the menu without glasses or reaches for their phone in their pocket. The difference between those two outcomes is decided in the workup room, not the operating theatre.
Double biometry, performed routinely, contributes to four outcomes that patients can feel:
- Lower enhancement risk. The patient is less likely to require laser correction or lens exchange after surgery because the original lens calculation was correct first time.
- Confident premium IOL selection. Trifocal, toric, and EDOF lenses are unforgiving of measurement error. Trustworthy biometry is what makes premium IOL surgery rational to offer.
- Toric planning that holds up. Toric IOLs rely on accurate axis and magnitude of corneal astigmatism, which requires both the keratometric value from the biometer and the full topographic map from the OCT.
- Honest pre-operative discussion. We can tell the patient what we are aiming for, what we expect, and what we will do if the outcome falls outside the target range, because the foundation those statements rest on has been independently verified.
Most clinics do not even track their enhancement rate. Enhancement rates reflect refractive planning quality more than they reflect surgical technique. Large-cohort outcome data confirms that the residual refractive error after modern optical-biometry-guided cataract surgery should sit close to zero on average, with 95% reproducibility intervals of approximately ±1 D⁸. Anything wider than this benchmark is, in our reading, a measurement problem more than a surgical one.
At Blue Fin Vision®, refractive precision is treated as a measurable outcome rather than a marketing slogan.
Why This Is Rare
If double biometry is so clinically obvious, why is it not standard practice everywhere? The honest answer is operational, not clinical.
- Cost. Two biometers cost roughly twice as much as one biometer. For a clinic that performs limited cataract volume, the second device is difficult to justify economically.
- Clinic footprint. Two large diagnostic machines in the same workup room is a non-trivial space constraint, especially in central London where every square foot is expensive.
- Workflow complexity. Double biometry adds time to every patient visit, not just complex cases. That time has to be designed into the appointment, not borrowed from it.
- Training. Two devices means two device-specific protocols, two sets of failure modes to recognise, and two output formats to interpret. The staff and surgeon both need to be fluent in both.
Our response has been to design the Blue Fin Vision® preoperative ecosystem around compact, complementary instrumentation. The Lenstar LS900 and the REVO FC sit alongside an autorefractor and slit lamp in a configuration small enough to fit in a single consulting room. The full preoperative biometric workup, including topography, anterior segment OCT, and posterior segment OCT screening, is completed without the patient leaving the chair.
The challenge in modern ophthalmology is not simply owning more machines. It is creating a diagnostic ecosystem that delivers maximal information with minimal compromise.

Beyond Biometry: The Wider Blue Fin Vision® Philosophy
Double biometry sits inside a broader operational philosophy at Blue Fin Vision®. It is not an isolated test. It is one visible expression of a culture that treats refractive precision as a systems problem, not a moment-of-surgery problem.
Other expressions of the same philosophy in our preoperative workup include:
- Posterior segment OCT screening for every patient considered for premium IOL surgery, to identify macular pathology that would limit the visual benefit of a trifocal or EDOF implant before the patient pays for one.
- Full anterior and posterior corneal topography on every patient, not only those with clinically suspicious K-readings. Subtle posterior keratoconic change is invisible to keratometry alone.
- On-site lens inventory across a full range of monofocal, monofocal-plus, EDOF, trifocal and toric IOLs, so that the lens chosen during the consultation is the lens implanted at surgery, with no substitution pressure on the day.
- Six consecutive years of audited National Ophthalmology Database (NOD) outcomes published by the operating surgeon, including a posterior capsule rupture rate of approximately 0.2% against a national benchmark of approximately 0.79%.
- Enhancement policy defined and disclosed before surgery, not negotiated afterwards. Patients know what we offer, what the timeline is, and what the cost is, before they sign anything.
Double biometry is not an isolated test. It is one visible expression of a wider culture of refractive precision.
Conclusion
Cataract surgery in 2026 is held to refractive-surgery standards, and patients are right to hold it to those standards. The technology to plan and execute a precise refractive outcome exists, is well validated, and has been for more than a decade. The question is not whether the tools work. The question is whether a clinic chooses to build its workflow around them.
At Blue Fin Vision®, we have made that choice. Every patient receives biometry on two independent platforms, using two different physical technologies, with independent confirmation of the refractive plan before surgery is booked. We do this routinely. We do this for the patient with a 23 mm normal axial length, no astigmatism and no prior refractive surgery, just as much as for the -12 D high myope with a previous LASIK procedure.
Double biometry does not replace modern IOL calculation methodology. It complements it. Contemporary formulae (Barrett Universal II, Hill-RBF, Olsen, Kane and Hoffer QST) have substantially reduced average prediction error compared with their predecessors⁷, and they are the calculation engine we run. But every formula in modern use is fed by the biometric data it is given. Two independent confirmations of that data are what allow a modern formula to perform at its best.
The patient does not see this workflow. They see the outcome. And the outcome, confident spectacle independence, predictable refractive results, and a low enhancement rate, is what the workflow was designed to produce.
Read more on whether you will still need glasses after premium lens surgery.
In modern cataract surgery, precision is not luck. It is the result of systems deliberately designed to reduce uncertainty.
References
- Sikorski BL, Suchon P. OCT Biometry (B-OCT): a new method for measuring ocular axial dimensions. J Ophthalmol. 2019;2019:9192456. doi:10.1155/2019/9192456
- Domínguez-Vicent A, Venkataraman AP, Dalin A, Brautaset R, Montés-Micó R. Repeatability of a fully automated swept-source optical coherence tomography biometer and agreement with a low coherence reflectometry biometer. Eye Vis (Lond). 2023;10(1):24. doi:10.1186/s40662-023-00343-4
- Jasvinder S, Khang TF, Sarinder KKS, Loo VP, Subrayan V. Agreement analysis of LENSTAR with other techniques of biometry. Eye (Lond). 2011;25(6):717-724. doi:10.1038/eye.2011.28
- Cruysberg LPJ, Doors M, Verbakel F, Berendschot TTJM, De Brabander J, Nuijts RMMA. Evaluation of the Lenstar LS 900 non-contact biometer. Br J Ophthalmol. 2010;94(1):106-110. doi:10.1136/bjo.2009.161729
- Hoffer KJ, Shammas HJ, Savini G. Comparison of 2 laser instruments for measuring axial length. J Cataract Refract Surg. 2010;36(4):644-648. doi:10.1016/j.jcrs.2009.11.007
- Norrby S. Sources of error in intraocular lens power calculation. J Cataract Refract Surg. 2008;34(3):368-376. doi:10.1016/j.jcrs.2007.10.031
- Kane JX, Van Heerden A, Atik A, Petsoglou C. Intraocular lens power formula accuracy: comparison of 7 formulas. J Cataract Refract Surg. 2016;42(10):1490-1500. doi:10.1016/j.jcrs.2016.07.021
- Miele A, Fumagalli C, Abbruzzese G, Savastano A, Rizzo S, Giansanti F, Virgili G. Biometric refractive error after cataract and retina surgery: a systematic review and a benchmark proposal. Eye (Lond). 2021;35(7):1810-1817. doi:10.1038/s41433-021-01464-7
- Kanclerz P, Hoffer KJ, Przewłócka K, Savini G. Comparison of the upgraded Revo NX with the IOLMaster 700 and the Lenstar. J Cataract Refract Surg. 2021;47(7):859-864. doi:10.1097/j.jcrs.0000000000000541
ABOUT THE AUTHOR
Mr Mfazo Hove
Consultant Ophthalmic Surgeon
MBChB MD FRCOphth CertLRS
Mr Mfazo Hove is a Consultant Ophthalmic Surgeon with experience spanning more than 57,000 procedures. He completed 6.5 years of specialist training at Moorfields Eye Hospital and served for five years as a consultant at the Western Eye Hospital, Imperial College Healthcare NHS Trust. He is the founder of Blue Fin Vision®, a consultant-led private ophthalmology practice operating across London, Essex, and Hertfordshire. His clinical expertise encompasses advanced cataract surgery, refractive lens replacement, laser vision correction, and implantable Collamer lenses (ICL).
A ZEISS Key Opinion Leader, Mr Hove is a respected international speaker with five invited engagements across seven cities in 2026:
- ZEISS China tour (Changsha, Shanghai, and Hangzhou, April – ZEISS APAC User Meeting)
- RCOphth Annual Congress – May – Manchester
- ZEISS EMEA User Meeting (Istanbul)
- ZEISS Lausanne User Meeting (Lausanne)
- European Society of Cataract and Refractive Surgeons Annual Congress (ESCRS, London)
Related Topics
Understanding Biometry and Why It Matters
The Two-Device Approach and the Technology Behind It
Outcomes, Premium Lenses and Enhancement Risk
Schedule Your Consultation Today
If you are considering cataract surgery or refractive lens exchange and want a measurement process built around independent confirmation, you can book a consultation to discuss your options with our team. Blue Fin Vision® is a consultant-led UK clinic with documented outcomes and centres across London, Hertfordshire and Essex, including our flagship clinic on Harley Street, alongside Weymouth Street, Chelmsford, Hatfield and Chase Lodge Hospital in North West London.

