
The Cataract Was Too Dense for Optical Biometry, What Happens Next?
- Posted
- Medically Reviewed by: Mr Mfazo Hove, Consultant Ophthalmic Surgeon
- Author: Mr Mfazo Hove
- Published: June 10, 2026
- Last Updated: June 10, 2026
Modern cataract surgery is often presented as a highly automated process. Patients are told that sophisticated scanners measure the eye, computers calculate the lens implant power, and surgery proceeds with remarkable precision. In many cases, that is true.
However, real-world cataract surgery is not always straightforward.
Occasionally, a patient presents with a cataract so dense that modern optical scanners cannot reliably measure the eye at all. When this happens, the process moves beyond simple automation and becomes heavily dependent on clinical judgement, interpretation, experience, and robust safety systems.
At Blue Fin Vision®, this is precisely where consultant-led care matters most.
Why Accurate Measurements Matter in Cataract Surgery
Before cataract surgery, surgeons must calculate the power of the intraocular lens (IOL) that will replace the cloudy natural lens. One of the most important measurements is the axial length (AL), the distance from the front of the eye to the retina.
Even very small inaccuracies can affect the final refractive outcome. An axial length error of just 0.1 mm can produce approximately 0.25 to 0.30 dioptres of refractive error after cataract surgery in an average eye.¹ ² Larger errors can significantly affect whether a patient remains glasses-independent, a particular concern when premium intraocular lenses are being implanted.⁵
Modern cataract surgery therefore relies heavily on optical biometry devices, which use light-based technology to measure the eye with extraordinary precision. In routine cases, these devices are highly accurate and reproducible.³ ⁷
But they still have limitations.
When Dense Cataracts Defeat the Machine
Certain cataracts, particularly dense posterior subcapsular cataracts (PSC) or advanced brunescent cataracts, scatter and absorb light so severely that optical biometry becomes difficult or impossible.
Instead of obtaining a clean retinal signal, the machine may produce:
- weak spikes,
- fragmented traces,
- inconsistent axial lengths,
- or entirely failed scans.
This creates an important clinical challenge.
The machine may still print a number, but that does not necessarily mean the number is trustworthy.
In some situations, accepting an inaccurate measurement without scrutiny can lead to a significant refractive surprise after surgery.
At Blue Fin Vision®, measurements are never accepted blindly simply because a machine generated them.
When optical biometry cannot deliver a reliable axial length, the fallback is ultrasound A-scan biometry, a contact or immersion technique that measures the eye using high-frequency sound waves rather than light.⁴ Sound penetrates the dense cataract where light cannot. But ultrasound A-scan is not a plug-and-play replacement; it is an operator-dependent test in which the surgeon and biometrist must interpret the waveform, recognise spurious readings, and decide which measurements to trust.⁶
Before examining this patient’s actual A-scans, it helps to know what a reliable trace should look like.
Read more: What type of cataract do you have?
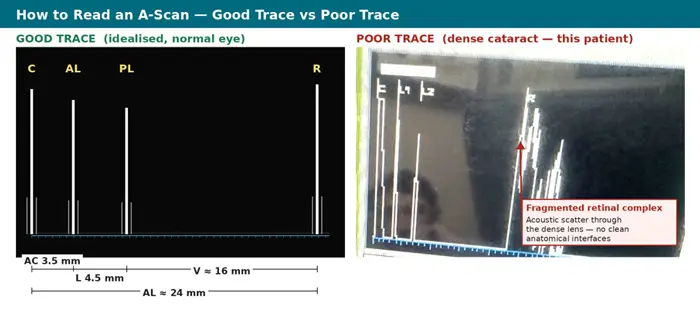
Figure 1. The two anatomies of an A-scan. A reliable trace (left) produces four distinct spikes at the cornea (C), anterior lens capsule (AL), posterior lens capsule (PL), and retina (R), with the component distances, anterior chamber (AC), lens thickness (L), vitreous chamber (V), and total axial length (AL), cleanly recoverable. A dense cataract (right) scatters and absorbs the ultrasound signal, producing fragmented returns with no clean anatomical interfaces. No IOL formula can rescue this without expert interpretation.
Worked Example, A-Scan Biometry From a Single Patient
The two A-scan ultrasound traces below were obtained from one patient whose cataracts were too dense for reliable optical biometry. They illustrate exactly why interpretation, not automation, drives safety in complex cataract surgery.
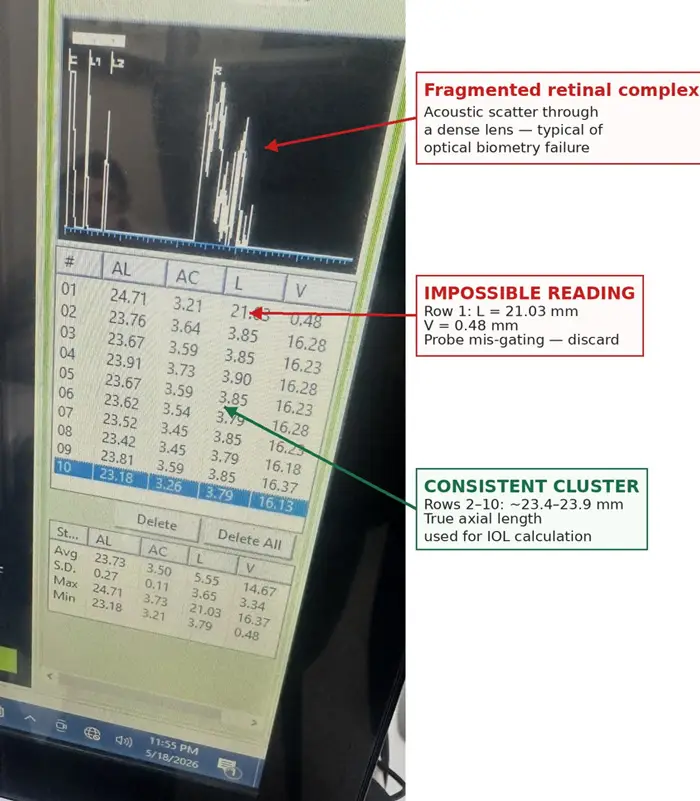
Figure 2. Right eye (OD), ten repeat A-scans. Mean axial length 23.73 mm, SD 0.27 mm. Annotations identify the anatomically impossible row 1 reading (probe mis-gating onto the wrong internal interface), the consistent cluster across rows 2 to 10 around 23.5 mm, the true axial length, and the fragmented retinal complex from acoustic scatter through a dense lens.

Figure 3. Left eye (OS), ten repeat A-scans. Mean axial length 23.26 mm, SD 0.17 mm. Annotations identify the row 10 outlier at 22.66 mm, the consistent cluster across rows 1 to 9 around 23.3 mm, the true axial length, and the noisy retinal complex characteristic of acoustic scatter through the dense lens.
What the surgeon must do
- Recognise that Figure 2 reading 1 is not a real eye, it must be discarded, not averaged.
- Identify the consistent cluster (around 23.6 to 23.8 mm OD and 23.3 mm OS) as the most plausible true axial length.
- Cross-check against inter-eye symmetry, corneal power, and pre-cataract refraction where available.
- Select an IOL calculation formula appropriate to the eye type and proceed only when confidence is sufficient.
The teaching point: the machine generated numbers. Some of those numbers were correct. One was anatomically impossible. None of that is apparent without a trained eye reading the trace.
In this case, surgery proceeded safely the following day using carefully interpreted ultrasound biometry after optical biometry failed due to the density of the cataract.
Where feasible, immersion A-scan biometry is preferred in complex eyes because it avoids the corneal compression artefact associated with the contact technique.
Why Repeating Measurements Is Essential
When optical or ultrasound biometry quality is poor, repeat measurements become critically important.
Rather than relying on a single scan, experienced surgeons look for:
- consistency between repeated readings,
- physiological plausibility,
- agreement between both eyes,
- waveform quality,
- correlation with refraction and clinical findings,
- and identification of obvious outliers.
In dense cataracts, it is common to obtain multiple readings with a few values that clearly do not fit the overall pattern.
For example:
- one measurement may appear significantly longer than all others,
- another may be abnormally short,
- while the majority cluster within a narrower, more believable range.
The challenge is not simply averaging numbers.
The challenge is understanding which numbers should not be trusted.
Experience is what separates a salvageable scan from a refractive surprise.
Read more on fixing post-cataract refractive error.

Why Human Judgement Still Matters
Artificial intelligence, automation, and advanced diagnostics have transformed cataract surgery. However, technology still requires interpretation.
A dense cataract may prevent the scanner from identifying the retina accurately, causing the device to mistake internal reflections or noise for the true retinal signal.
An experienced cataract surgeon recognises these patterns.
This involves:
- analysing waveform morphology,
- assessing signal reliability,
- comparing inter-eye symmetry,
- correlating measurements with corneal power and refraction,
- and deciding whether additional techniques are required.
Sometimes ultrasound biometry becomes necessary when optical methods fail completely. In other cases, repeated optical scans combined with careful clinical interpretation provide sufficient confidence to proceed safely.
In difficult cataracts, the outcome depends less on the scanner itself and more on the systems and expertise interpreting the data.
The Difference Between Data Collection and Data Interpretation
One of the misconceptions in modern cataract surgery is that the machine itself creates the outcome.
In reality, the machine only collects information.
The surgeon must still determine whether that information is reliable, whether the measurements make physiological sense, whether the readings correlate with the clinical picture, and how much uncertainty exists before surgery proceeds.
This distinction becomes particularly important in complex eyes, where measurement quality cannot be taken for granted and where every value must be cross-checked before it is allowed to drive an IOL calculation.
Why Dense Cataracts Often Need Experienced Surgeons
Many patients assume cataract surgery is identical everywhere because the operation itself is common.
However, not all cataracts are routine.
Dense cataracts increase complexity before surgery even begins. Poor measurements, limited visibility, advanced lens density, weak zonules, small pupils, and higher complication risk all require greater judgement and adaptability.
In advanced cataract surgery, volume builds the pattern recognition that no machine can replace.
A surgeon who regularly manages advanced cataracts develops pattern recognition that cannot simply be automated.
They become familiar with:
- suspicious measurement patterns,
- unreliable scans,
- difficult anatomy,
- and contingency planning when technology is imperfect.
Experience is what makes deviation from the ideal pathway recoverable rather than dangerous.

Technology Is Powerful, But Systems Matter More
Modern ophthalmology has achieved extraordinary technological progress. Optical biometers, OCT imaging, advanced formulas, premium intraocular lenses, and AI-assisted calculations have dramatically improved outcomes for patients worldwide. But technology alone is not enough. The safest outcomes occur when advanced technology meets rigorous measurement protocols, consultant interpretation, repeat verification, and systems designed to reduce uncertainty.⁵ At Blue Fin Vision®, this philosophy underpins the entire cataract pathway.
Because in complex cataract surgery, the critical question is not whether the machine produced a number.
The critical question is whether the number is correct.
References
- Olsen T. Calculation of intraocular lens power: a review. Acta Ophthalmologica Scandinavica. 2007;85(5):472-485.
- Hill W. Axial length measurement accuracy and intraocular lens calculation. Current Opinion in Ophthalmology. 2008;19(1):13-17.
- Findl O, Drexler W, Menapace R, Georgopoulos M, Rainer G, Hitzenberger CK, Fercher AF. Improved prediction of intraocular lens power using partial coherence interferometry. Journal of Cataract and Refractive Surgery. 2001;27(6):861-867.
- Wang JK, Hu CY, Chang SW. Intraocular lens power calculation using ultrasound biometry in eyes with dense cataracts. Journal of Cataract and Refractive Surgery. 2008;34(5):847-852.
- Norrby S. Sources of error in intraocular lens power calculation. Journal of Cataract and Refractive Surgery. 2008;34(3):368-376.
- Byrne SF. A-Scan Axial Length Measurements: A Handbook for IOL Calculations. Mars Hill, NC: Grove Park Publishers; 1995.
- Connors R, Boseman P, Olson RJ. Accuracy and reproducibility of biometry using partial coherence interferometry. Journal of Cataract and Refractive Surgery. 2002;28(2):235-238.
ABOUT THE AUTHOR
Mr Mfazo Hove
Consultant Ophthalmic Surgeon
MBChB MD FRCOphth CertLRS
Mr Mfazo Hove is a Consultant Ophthalmic Surgeon with experience spanning more than 57,000 procedures. He completed 6.5 years of specialist training at Moorfields Eye Hospital and served for five years as a consultant at the Western Eye Hospital, Imperial College Healthcare NHS Trust. He is the founder of Blue Fin Vision®, a consultant-led private ophthalmology practice operating across London, Essex, and Hertfordshire. His clinical expertise encompasses advanced cataract surgery, refractive lens replacement, laser vision correction, and implantable Collamer lenses (ICL).
A ZEISS Key Opinion Leader, Mr Hove is a respected international speaker with five invited engagements across seven cities in 2026:
- ZEISS China tour (Changsha, Shanghai, and Hangzhou, April – ZEISS APAC User Meeting)
- RCOphth Annual Congress – May – Manchester
- ZEISS EMEA User Meeting (Istanbul)
- ZEISS Lausanne User Meeting (Lausanne)
- European Society of Cataract and Refractive Surgeons Annual Congress (ESCRS, London)
Related Topics
Understanding Why Eye Scans Fail
The Backup Measurement Technique
Discuss Your Cataract Surgery Options
If you or someone you care for has been told a cataract is particularly dense or complex, the quality of the measurement and the experience interpreting it matter just as much as the surgery itself. At Blue Fin Vision®, complex cataracts are managed by consultants who interpret biometry personally rather than accepting a machine reading at face value.
View patient feedback on our Wall of Love
To talk through your options, book a consultation with our team. You will be trusting your vision to a consultant-led UK clinic with documented outcomes and locations across London, Hertfordshire, and Essex.


