
- Medically Reviewed by: Mr Mfazo Hove, Consultant Ophthalmic Surgeon
- Author: Mr Mfazo Hove
- Published: July 13, 2026
- Last Updated: July 15, 2026
Why timing is not always causation, and why independent second opinions matter.
The scan before surgery was clear. A year later, it was not.
A new problem had appeared after eye surgery, and the obvious question was whether the surgery had caused it. That question is fair. But in medicine, timing is not the same as causation. Some problems are caused by surgery. Some are revealed by surgery. Some develop coincidentally during follow-up. Knowing the difference matters, for the patient, for the surgeon, and for the standard of care.
This is exactly where an independent second opinion earns its place.
A Routine Case, Until It Was Not
One patient came to me for lens replacement surgery. Routine in every respect but one. At the initial consultation I had reservations about their suitability for a trifocal lens, and I said so. Rather than push a decision, I left the consultation open and asked them to take time to reflect. They returned a few weeks later, having decided that they wanted the spectacle independence a premium lens can offer, and we proceeded only after a full discussion of glare, haloes, starburst and the need for neuroadaptation.
From the second day after surgery they found the glare and haloes difficult. We supported them closely through the adaptation window, but the symptoms did not settle to their satisfaction. Some months later, together, we agreed on a trifocal to monofocal lens exchange in one eye. The lens exchange itself was uneventful. When I reviewed the patient afterwards and scanned the macula to check for cystoid macular oedema, which is a routine and expected thing to look for after any intraocular surgery, the scan showed something that had not been present on the pre-operative macular OCT: an epiretinal membrane.
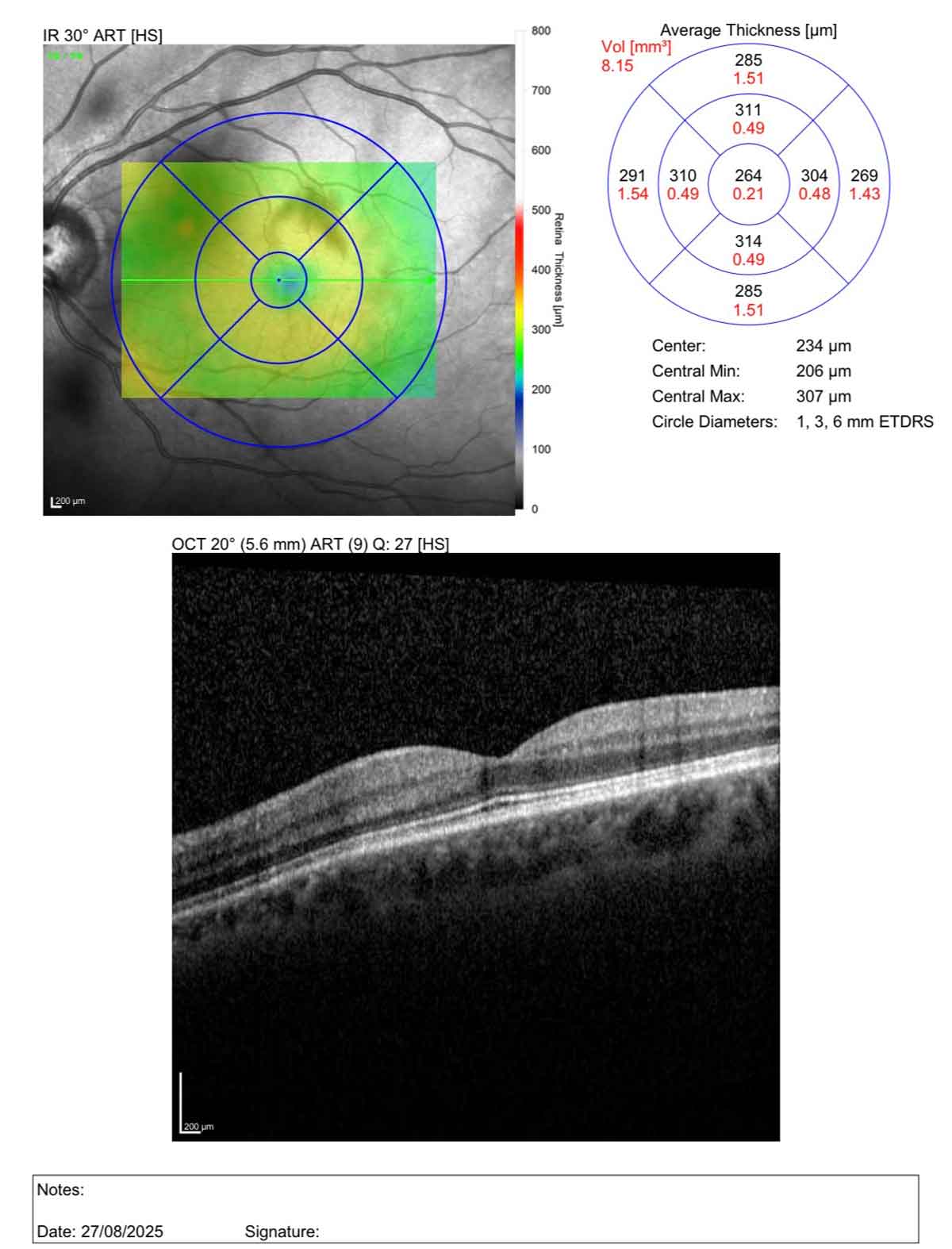
Macular OCT before lens replacement surgery, 27 August 2025. Central retinal thickness 234 microns, with a normal foveal contour and no epiretinal membrane present.
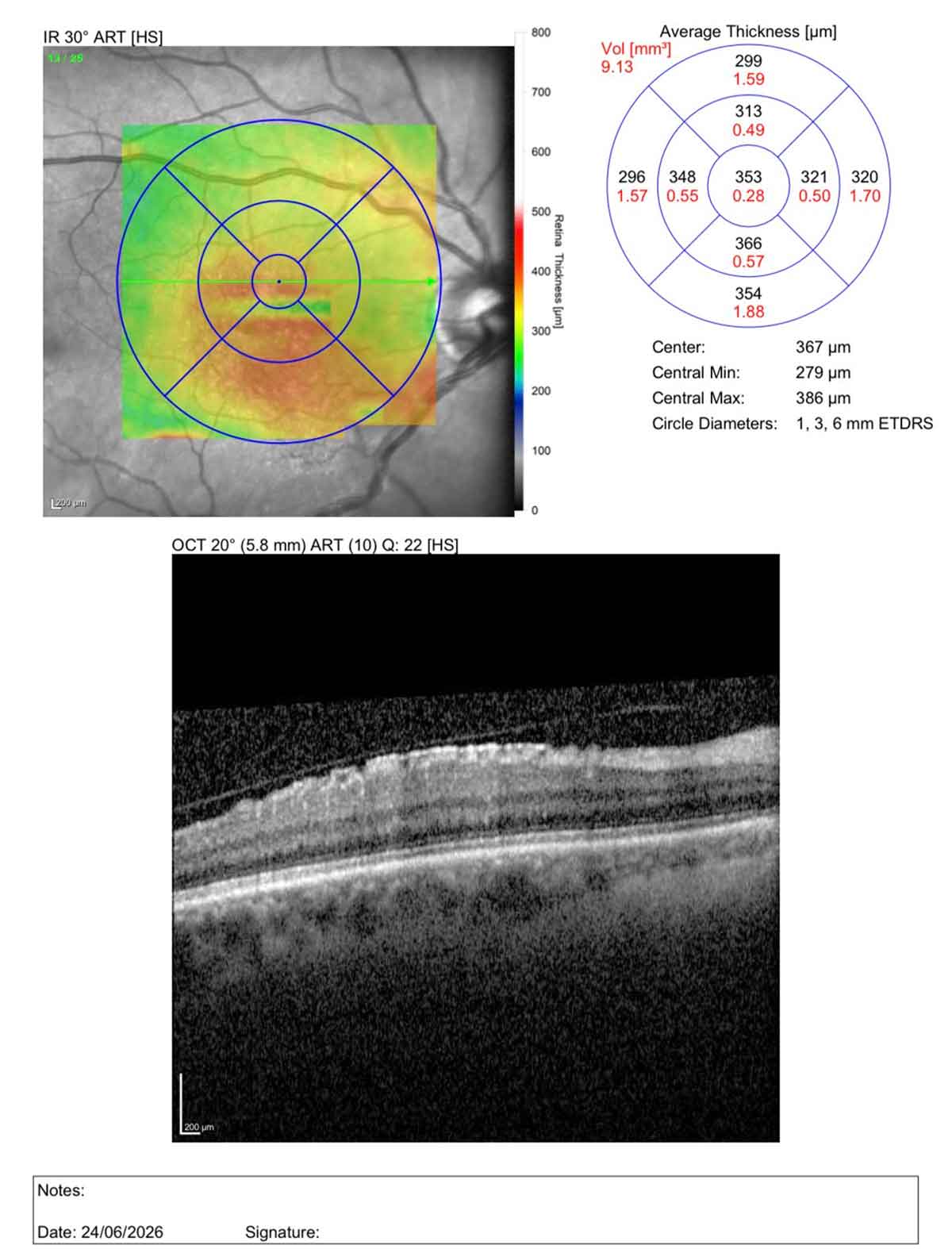
Macular OCT approximately one year later, 24 June 2026, following lens replacement and a subsequent trifocal to monofocal lens exchange. Central retinal thickness has increased to 367 microns, and a fine epiretinal membrane is now visible at the macular surface.
And there the difficult conversation began. If the membrane was not obvious before and is visible now, did the surgery cause it?
Cause and Coincidence
This is one of the most misunderstood ideas in surgical medicine, and it is entirely understandable. When something appears after an operation, the mind reaches for the operation as the explanation. But sequence is not the same as cause. Not every problem that follows eye surgery has been produced by it.
Some things genuinely are related to the surgery, and we should say so plainly. Cataract and lens replacement surgery accelerates the natural separation of the vitreous gel from the retina, a posterior vitreous detachment.¹ A posterior vitreous detachment happens to most people eventually without any surgery at all, but the operation can bring it forward. In a small number of eyes that separation can, in turn, cause new floaters, a retinal tear or, rarely, a retinal detachment. That is a recognised, if uncommon, sequence, and it is one we counsel on and watch for.
An epiretinal membrane is a different matter. It is an age-related condition in which a fine sheet of cells forms on the surface of the macula, and it is common in the older population.² ³ An epiretinal membrane can be present, unnoticed, before any surgery, but it can also appear during a period of follow-up, developing as part of age-related change at the interface between the vitreous and the retina.⁴ ⁵
That is what matters in this case, and I want to be plain about it rather than tidy it away. The pre-operative macular scan did not show an epiretinal membrane. The membrane became visible over the year that followed, a year in which the patient was managed for glare and haloes and underwent a second operation, a trifocal to monofocal lens exchange. So the membrane appeared after not one but two intraocular procedures, and it was not there when the journey began. That timing naturally raises the question of causation, and it is a fair question to ask. But timing alone is not causation. Lens replacement surgery does not cause an epiretinal membrane to develop in an otherwise healthy macula. What surgery can do is make the visual consequences of a membrane more noticeable, or increase the chance of associated cystoid macular oedema.⁶ ⁷ That is not the same as creating the membrane.
These are genuinely fine distinctions. They are difficult to hold onto when you are the patient living with the symptoms, and no amount of explanation from the operating surgeon ever fully removes the natural suspicion that the surgeon has an interest in the answer.

Where a Second Opinion Earns Its Place
This is exactly the situation in which an independent second opinion earns its place. I had reviewed the patient, identified the membrane and explained my view of how it had arisen. But when the difficult question is whether the surgeon’s own operation is to blame, the surgeon is not the ideal person to have the last word. So I have recommended that the patient see an independent retinal specialist, with no connection to the surgery, for their own assessment of the membrane and its management. That opinion is theirs to seek, and I have made clear why I think it is worth having.
This is also consistent with professional duty: the General Medical Council requires doctors to be open and honest with patients when something goes wrong or when a concern is raised, a principle known as the duty of candour.⁸
An independent second opinion does three things that the treating surgeon cannot do alone. It reassures the patient, because the message no longer depends on the person who performed the operation. It protects the relationship, because trust survives far better when a neutral voice confirms the account. And it upholds the standard, because a surgeon who is willing to invite outside scrutiny, and to fund it where a problem stems from their own care, is a surgeon who is confident the work was sound.
At Blue Fin Vision® we further support this commitment through comprehensive documentation: consultations are recorded with consent, pre-operative diagnostics include double biometries, and all surgeries are fully recorded. These objective records ensure clarity for both patient and surgeon when reviewing outcomes, supporting informed discussions about cause and coincidence without relying solely on recollection.
What We Cover, and Why the Boundary Matters
At Blue Fin Vision® we are deliberately, and sometimes expensively, comprehensive about caring for the complications of the treatment we ourselves provide. That commitment is concrete:
- Dry eye after laser vision correction. We provide lubricants without limit, for as long as they are needed, rather than capping supply at a set number of bottles.
- Recalcitrant dry eye. We prescribe topical ciclosporin, an effective but costly drug, at no charge to the patient, absorbing that cost rather than passing it on.
- A dropped nucleus during cataract or lens replacement surgery. We hold our own in-house vitreoretinal cover, so this rare intraoperative complication is dealt with promptly within our service rather than outsourced with delay.
- Implantable collamer lens patients. We provide our Lifetime Monitoring Protocol™, with regular endothelial cell counts and vault scans, and if a cataract later develops we cover its treatment in full for the first two years and half of the cost for up to ten years.
- Residual refractive error after refractive surgery. If a laser or lens enhancement is needed to fine-tune the result, it is fully covered for our self-pay laser vision correction, implantable collamer lens and refractive lens replacement patients, under our enhancement policy.
- A complication of our own treatment that needs an outside view. Where a genuine complication warrants it, such as corneal haze after PRK, a recognised laser-related complication, we arrange the independent opinion and we pay for it.
None of this is generosity for its own sake, and none of it is marketing. It is simply what it means to stand behind your own work. These commitments cost us real money and time, by design, because the outcomes of what we do are ours to own. Together they are part of what we call the Blue Fin Vision® Advantage.
But the same principle that makes us generous also draws a line, and that line is not a piece of small print. It is the other half of the same commitment. We stand behind the complications of our surgery according to clear, published clinical policies. We do not, however, accept causal or financial responsibility for an age-related condition such as an epiretinal membrane simply because it happened to be detected after an operation, when the available clinical evidence does not support the operation as the cause. A membrane found after lens replacement should not automatically be treated as a complication of that surgery, just as a retinal problem found after pterygium surgery would not automatically be treated as a complication of pterygium surgery. In situations like these we will always explain what we have found and recommend the right independent specialist, but the investigation and ongoing care of a coincidental condition belong to the patient’s wider eye care, not to our surgical complication cover. Confusing a coincidental problem with a caused one would, in the end, weaken the care we can offer to everyone. Honest scope is what makes generous cover sustainable.
The Clinical Takeaway
Patients struggle, reasonably, with cause and coincidence, and the burden of resolving that honestly sits with us, not with them. The answer is not to defend our own work more loudly. It is to invite an independent view when causation is disputed, to fund that view where the issue plausibly relates to our treatment, and to be equally clear about what we will stand behind and what we will not. We do not need fewer conversations about complications. We need more second opinions.
References
- Mirshahi A, Hohn F, Lorenz K, Hattenbach LO. Incidence of posterior vitreous detachment after cataract surgery. Journal of Cataract and Refractive Surgery. 2009;35(6):987-991.
- Fraser-Bell S, Guzowski M, Rochtchina E, Wang JJ, Mitchell P. Five-year cumulative incidence and progression of epiretinal membranes: the Blue Mountains Eye Study. Ophthalmology. 2003;110(1):34-40.
- Bu SC, Kuijer R, Li XR, Hooymans JMM, Los LI. Idiopathic epiretinal membrane. Retina. 2014;34(12):2317-2335.
- Kwon S, Kim B, Jeon S. Risk factors for onset or progression of epiretinal membrane after cataract surgery. Scientific Reports. 2021;11:14808.
- Fong CSU, Mitchell P, Rochtchina E, Hong T, de Loryn T, Wang JJ. Incidence and progression of epiretinal membranes in eyes after cataract surgery. American Journal of Ophthalmology. 2013;156(2):312-318.e1. doi:10.1016/j.ajo.2013.03.022.
- Yonekawa Y, Kim IK. Pseudophakic cystoid macular edema. Current Opinion in Ophthalmology. 2012;23(1):26-32.
- Hardin JS, Gauldin DW, Soliman MK, Chu CJ, Yang YC, Sallam AB. Cataract surgery outcomes in eyes with primary epiretinal membrane. JAMA Ophthalmology. 2018;136(2):148-154. doi:10.1001/jamaophthalmol.2017.5849.
- General Medical Council. Openness and honesty when things go wrong: the professional duty of candour. Manchester: GMC; 2015 (updated 2022).
ABOUT THE AUTHOR
Mr Mfazo Hove
Consultant Ophthalmic Surgeon
MBChB MD FRCOphth CertLRS
Mr Mfazo Hove is a Consultant Ophthalmic Surgeon with experience spanning more than 57,000 procedures. He completed 6.5 years of specialist training at Moorfields Eye Hospital and served for five years as a consultant at the Western Eye Hospital, Imperial College Healthcare NHS Trust. He is the founder of Blue Fin Vision®, a consultant-led private ophthalmology practice operating across London, Essex, and Hertfordshire. His clinical expertise encompasses advanced cataract surgery, refractive lens replacement, laser vision correction, and implantable Collamer lenses (ICL).
A ZEISS Key Opinion Leader, Mr Hove is a respected international speaker with five invited engagements across seven cities in 2026:
- ZEISS China tour (Changsha, Shanghai, and Hangzhou, April – ZEISS APAC User Meeting)
- RCOphth Annual Congress – May – Manchester
- ZEISS EMEA User Meeting (Istanbul)
- ZEISS Lausanne User Meeting (Lausanne)
- European Society of Cataract and Refractive Surgeons Annual Congress (ESCRS, London)


