
Patient Experience
“The lens replacement surgery was complicated by my prior lasik procedure to both eyes 10 years prior … I found the information supplied was accurate and helpful.”
Clinical Explanation
Standard biometry devices do not measure the full thickness of the cornea directly. They measure the front surface and then estimate the cornea’s total focusing power using a fixed mathematical assumption about the ratio between its front and back surfaces, a ratio that holds true in eyes that have never been operated on.
The scanner only sees the front of the cornea and assumes the back matches it. Laser surgery changes the front but not the back, so the old assumption no longer fits.
Myopic LASIK and PRK flatten the front surface of the cornea but leave the back surface largely unchanged. This breaks the assumed front-to-back ratio. As a result, standard devices overestimate the true corneal power, the formula then selects a lens that is too weak, and the eye ends up more long-sighted than intended, the classic “hyperopic surprise” after cataract surgery in a previously myopic-LASIK eye. (Eyes treated for long sight show the opposite tendency.) Laser treatment also disturbs the prediction of where the new lens will finally sit, adding a second source of error.
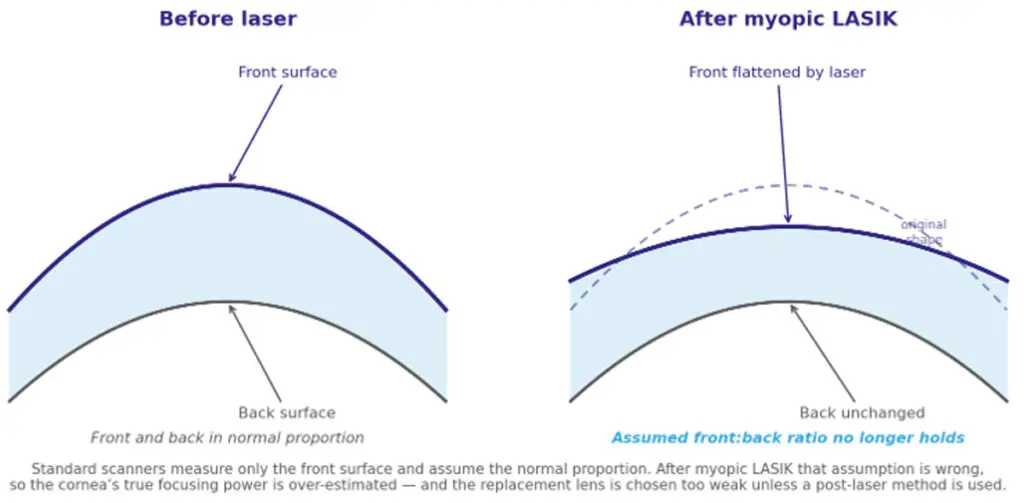
Figure 1. Why standard lens-power calculation under-reads a post-LASIK cornea, the front surface is flattened by the laser while the back is unchanged, breaking the front-to-back ratio that ordinary scanners assume.
This is why specialised approaches exist: history-based methods that use the pre-laser prescription; no-history methods such as the Haigis-L and Barrett True-K formulae that work without it; measurement-based methods such as total keratometry that attempt to capture the back surface directly; and intraoperative aberrometry, which checks the eye’s refraction during surgery. No single method is reliable alone; accuracy comes from applying several and reconciling them.
Structured Context
Applies to: eyes with previous excimer laser correction (LASIK, PRK, LASEK). The direction of error is predictable, previous short-sight treatment tends toward a long-sighted surprise, and previous long-sight treatment toward a short-sighted one.
Does not apply to: unoperated corneas, where conventional formulae remain the standard; and radial keratotomy, which alters the cornea by a different mechanism and is handled separately. None of these methods removes the need for clinical judgement in the individual eye.
Published Evidence
The underlying error was characterised more than two decades ago: standard calculation systematically underestimates the required lens power after myopic photorefractive surgery.¹ Subsequent reviews catalogued the history-based, no-history and measurement-based methods developed in response,² ³ including the widely used Haigis-L no-history formula⁴ and total-keratometry measurement of the cornea.⁵ Comparative studies in post-laser eyes show meaningful differences between methods,⁶ with the Barrett True-K among the most accurate currently available.⁷ Even so, national assessment confirms that refractive outcomes in these eyes remain less accurate than in unoperated eyes, however carefully the calculation is performed.⁸
Surgeon Interpretation
The post-laser cornea is, in our framework, a textbook structural source of outcome variability, a measurable, predictable departure from the assumptions ordinary biometry is built on. The principle we apply is simple: measure everything, and never trust a single number. We obtain the cornea’s power by more than one route, run several post-laser formulae in parallel, and treat agreement between them as the signal and disagreement as the instruction to look harder, including a direct check during surgery when the preoperative figures will not settle. The difficulty here is specific and well understood. The skill is not in any one formula; it is in holding several against each other and knowing which to believe.
Mr Mfazo Hove, Consultant Ophthalmic Surgeon.
Clinical Takeaway
The difficulty is specific, predictable and well understood: laser treatment breaks an assumption that ordinary lens-power calculation depends on. The solutions exist and work, but they must be used together, not relied on singly.
References
- Seitz B, Langenbucher A, Nguyen NX, Kus MM, Küchle M. Underestimation of intraocular lens power for cataract surgery after myopic photorefractive keratectomy. Ophthalmology. 1999;106(4):693-702. doi:10.1016/S0161-6420(99)90153-7
- Wang L, Koch DD. Intraocular lens power calculations in eyes with previous corneal refractive surgery: review and expert opinion. Ophthalmology. 2021;128(11):e121-e131. doi:10.1016/j.ophtha.2020.06.054
- Savini G, Hoffer KJ. Intraocular lens power calculation in eyes with previous corneal refractive surgery. Eye Vis (Lond). 2018;5:18. doi:10.1186/s40662-018-0110-5
- Haigis W. Intraocular lens calculation after refractive surgery for myopia: Haigis-L formula. J Cataract Refract Surg. 2008;34(10):1658-1663. doi:10.1016/j.jcrs.2008.06.029
- Wang L, Spektor T, de Souza RG, Koch DD. Evaluation of total keratometry and its accuracy for intraocular lens power calculation in eyes after corneal refractive surgery. J Cataract Refract Surg. 2019;45(10):1416-1421. doi:10.1016/j.jcrs.2019.05.020
- McCarthy M, Gavanski GM, Paton KE, Holland SP. Intraocular lens power calculations after myopic laser refractive surgery: a comparison of methods in 173 eyes. Ophthalmology. 2011;118(5):940-944. doi:10.1016/j.ophtha.2010.08.048
- Abulafia A, Hill WE, Koch DD, Wang L, Barrett GD. Accuracy of the Barrett True-K formula for intraocular lens power prediction after laser in situ keratomileusis or photorefractive keratectomy for myopia. J Cataract Refract Surg. 2016;42(3):363-369. doi:10.1016/j.jcrs.2015.11.039
- Pantanelli SM, Lin CC, Al-Mohtaseb Z, Rose-Nussbaumer JR, Santhiago MR, Steigleman WA 3rd, Schallhorn JM. Intraocular lens power calculation in eyes with previous excimer laser surgery for myopia: a report by the American Academy of Ophthalmology. Ophthalmology. 2021;128(5):781-792. doi:10.1016/j.ophtha.2020.10.031



