
Patient Experience
“I had cataracts in both eyes at early stage. The lens replacement surgery was complicated by my prior lasik procedure to both eyes 10 years prior. Two surgeons were not keen to proceed due to this complication. I found Mr Hove engaging and straight forward in his communication. He was clear of the risks but equally confident in his ability to proceed. Whilst scheduling the surgery was a bit involved the actual procedure was quick and straightforward. I found the information supplied was accurate and helpful. Mr Hove’s obvious talent as a surgeon was apparent and reassuring. My vision improved rapidly and I have now been discharged. I have no hesitation in recommending Mr Hove for this procedure.”
Trifocal lens surgery is usually possible after LASIK, so the real question is why one surgeon declines while another proceeds. The answer is almost always the lens: the result depends on which lens is chosen, and on whether the surgeon has direct, repeated experience implanting that specific lens in eyes that have already had laser correction. The case below, a verified patient who had been declined by two other surgeons, shows why that experience is the deciding factor.
The detail that matters clinically is the one this patient mentions almost in passing: two surgeons had already declined. That is common in this situation, and the reason is rarely the patient, it is the lens.
Clinical Explanation
Laser eye surgery for short-sightedness (myopic LASIK or PRK) works by flattening the centre of the cornea. That reshaping does two things that persist for life. First, it changes the optics of the cornea: myopic laser treatment measurably increases corneal spherical aberration and other higher-order aberrations, and the more correction that was originally applied, the larger that change tends to be.¹ The cornea is no longer the smooth, predictable surface the eye was born with.
Second, it makes the lens-power calculation far harder. Standard formulas assume a cornea that has never been operated on, so in post-laser eyes they systematically mis-predict, and specialised methods (such as the Barrett True-K formula) are required even to get the focal point close to target.² This is why scheduling and planning in these cases is, as this patient put it, “a bit involved.”
Now add a presbyopia-correcting lens on top of that altered cornea. A trifocal or diffractive lens splits incoming light to create three points of focus, near, intermediate and distance. Behind a cornea that has never been operated on, that works elegantly.
Behind a cornea already carrying extra aberration from previous laser treatment, the two optical systems interact. The visual quality the patient actually experiences then becomes lens-dependent in a way it never is in an eye that has not had surgery.³
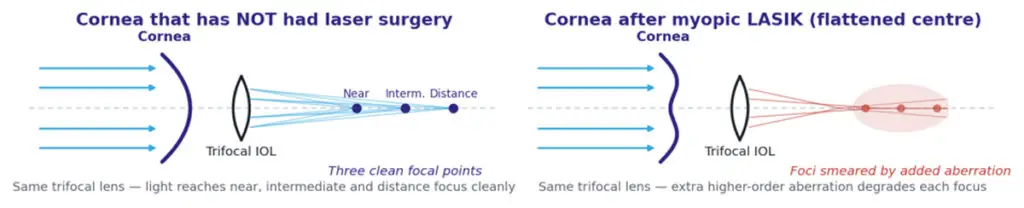
Figure 1. The same trifocal lens behind two different corneas. The lens that gives three clean focal points in an untouched eye can produce smeared, degraded focus behind a cornea flattened by previous myopic LASIK. Same lens; different cornea; different result.
The encouraging part is that the right lens, in the right hands, performs well. Published series of the ZEISS trifocal (AT LISA tri 839MP) implanted specifically in post-laser eyes report good distance and intermediate vision, acceptable near vision and high spectacle independence, in one series, around four in five patients needed no glasses at any distance.⁴ Compared directly against a monofocal lens in post-myopic-LASIK eyes, the trifocal delivered significantly better near vision with only a minimally different safety profile, provided patient selection was appropriate.⁵
Structured Context
Applies to: patients who have had previous myopic LASIK or PRK and now have early cataract or are considering lens replacement, and who would like to reduce or remove their dependence on glasses for near, intermediate and distance vision.
Does not apply to: eyes with an unstable or recently changing prescription, or any suggestion of corneal weakening (ectasia); significant dry eye, a large angle kappa or a decentred treatment zone, all of which can degrade multifocal performance; macular disease, significant glaucoma or other conditions where a presbyopia-correcting lens is not advisable; or a history of hyperopic (long-sight) laser treatment, which behaves differently again and needs separate assessment. In each of these situations the right answer may be a different lens, a monofocal target, or no surgery yet, which is exactly the judgement an experienced surgeon is there to make.
Published Evidence
Myopic laser treatment measurably increases corneal spherical aberration and other higher-order aberrations, in proportion to the original correction applied.¹ Standard lens-power formulae mis-predict in these eyes, and specialised methods such as the Barrett True-K are needed to bring the focal point close to target.² Behind an already-aberrated cornea, the optics of a diffractive lens interact with the corneal surface, so visual quality becomes lens-dependent in a way it is not in an unoperated eye.³ Even so, published series of the ZEISS trifocal (AT LISA tri 839MP) in post-laser eyes report good distance and intermediate vision and high spectacle independence,⁴ and direct comparison against a monofocal lens in post-myopic-LASIK eyes shows significantly better near vision with a minimally different safety profile when patient selection is appropriate.⁵
Surgeon Interpretation
“Why do other surgeons decline these cases? Almost always because the lens they routinely use, their default lens, cannot be relied upon to perform in an eye that has had laser surgery, and they know that a poor result here leads to a deeply dissatisfied patient. Declining is the safe choice for the surgeon. It is not the only choice for the patient.
Here is the uncomfortable truth about lens selection in this group: no single biometric or aberrometric measurement reliably tells you in advance which presbyopia-correcting lens will give a particular post-laser eye its best result. The corneas are individual, and the optics interact in ways a machine cannot fully predict. Lens choice in these eyes is led by experience and judgement, by knowing how a specific lens has actually behaved across many similar corneas, not by a number on a screen.
That is why I do not transfer a lens’s reputation in normal eyes onto a post-laser eye. A lens can give beautiful vision in a cornea that has never been touched and still disappoint behind a laser-treated one. In this group my lens of choice is the ZEISS trifocal (AT LISA tri 839MP), because I have implanted it repeatedly in laser-treated eyes and I have published, repeatable outcomes to stand behind.⁴ ⁵ Putting in a lens I could not predict risks stacking higher-order aberrations on an already-aberrated cornea, and compromising the very visual quality the patient came for.
So, if you have had laser surgery and you are being offered a premium lens, ask one question: ‘How many laser eye surgery patients have you implanted with the exact lens you are recommending to me, and what were their results?’ The answer will tell you more than any brochure.”
Mr Mfazo Hove, Consultant Ophthalmic Surgeon.
Even in experienced hands, post-laser trifocal surgery remains less predictable than surgery in an untouched cornea. That unpredictability is precisely why enhancement planning matters. At Blue Fin Vision®, patients undergoing complex post-laser lens surgery are covered by the Blue Fin Vision® Advantage and comprehensive enhancement policy: if further refinement is required, laser enhancement or a secondary “piggyback” lens correction is provided without additional surgeon fees to the patient.
Clinical Takeaway
Trifocal lens surgery after LASIK is possible in carefully selected eyes, but the result depends on the specific lens and the surgeon’s repeated experience with it in laser-treated corneas. A surgeon’s caution often reflects the limits of their default lens, not the limits of what is achievable.
References
- Kohnen T, Mahmoud K, Bühren J. Comparison of corneal higher-order aberrations induced by myopic and hyperopic LASIK. Ophthalmology. 2005;112(10):1692-1698.
- Abulafia A, Hill WE, Koch DD, Wang L, Barrett GD. Accuracy of the Barrett True-K formula for intraocular lens power prediction after laser in situ keratomileusis or photorefractive keratectomy for myopia. J Cataract Refract Surg. 2016;42(3):363-369.
- Alfonso JF, Madrid-Costa D, Poo-López A, Montés-Micó R. Visual quality after diffractive intraocular lens implantation in eyes with previous myopic laser in situ keratomileusis. J Cataract Refract Surg. 2008;34(11):1848-1854.
- Li QM, Wang F, Wu ZM, Liu Z, Zhan C, Chen BH, Sima J, Stieger K, Li SW. Trifocal diffractive intraocular lens implantation in patients after previous corneal refractive laser surgery for myopia. BMC Ophthalmol. 2020;20(1):293.
- Bilbao-Calabuig R, Ortega-Usobiaga J, Mayordomo-Cerdá F, Beltrán-Sanz J, Fernández-García J, Cobo-Soriano R. Trifocal versus monofocal intraocular lens implantation in eyes previously treated with laser in situ keratomileusis (LASIK) for myopia. Indian J Ophthalmol. 2024;72(Suppl 2):S254-S259.



