
- Medically Reviewed by: Mr Mfazo Hove, Consultant Ophthalmic Surgeon
- Author: Mr Mfazo Hove
- Published: May 27, 2026
- Last Updated: May 27, 2026
The intraocular lens you choose will define how you experience light, contrast, depth, and independence from glasses for the rest of your life. It is the single most consequential decision in cataract and refractive lens surgery, and the one most often reduced to marketing categories that obscure what actually matters.
Patients are typically presented with four tiers:
- Monofocal
- Monofocal plus
- EDOF (extended depth of focus)
- Trifocal
…and increasingly, the suggestion that you can “upgrade later” with a piggyback lens.
The reality is more demanding. Two patients can choose the same lens and describe entirely different visual experiences. Understanding why, and what that means for your decision, matters far more than the label on the box.
The Goal: Vision Freedom vs Optical Trade-Offs
Every IOL design is a compromise between three variables:
- Range of vision (distance, intermediate, near)
- Optical quality (contrast sensitivity)
- Dysphotopsia (haloes, glare, starbursts)
No lens eliminates these trade-offs. The clinical question is not which lens is “best.” It is which trade-off profile fits your eye, your lifestyle, and your tolerance.
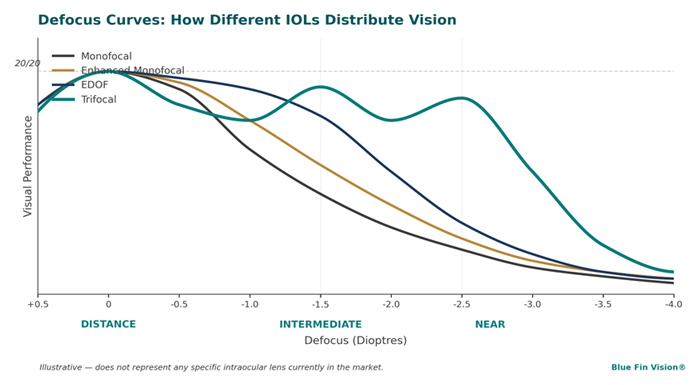
Figure 1. Defocus curves illustrate how each lens type distributes vision across distance, intermediate, and near. Higher curves represent better visual performance at that focal range. Trifocals provide three peaks (full range); EDOF lenses extend a single plateau into intermediate; enhanced monofocals modestly broaden the distance peak; standard monofocals concentrate performance at distance only.
Adapted from established defocus curve pedagogy. Schematic only and does not represent any specific intraocular lens platform.
Trifocal IOLs: Maximum Range, Maximum Optical Complexity
Trifocal lenses provide three focal points: distance, intermediate, and near. They achieve this by splitting incoming light using diffractive optics.¹
Modern platforms include the ZEISS AT LISA tri 839MP, the Alcon PanOptix, and the FineVision (PhysIOL). They differ in light distribution, defocus curve, and pupil dependence, but all share the same fundamental optical strategy.
What this means in practice:
- High rates of spectacle independence²
- Functional vision across all distances
- Higher incidence of haloes and glare, particularly at night³
The Critical Nuance
Trifocals are often described as the lens that “causes haloes.” This framing is incomplete.
The perception of haloes and glare is highly patient-specific. Neuroadaptation, pupil dynamics, ocular surface quality, and higher-order aberrations all influence how light is processed by the visual system.⁴
Two patients with identical trifocal implants can report:
- “Perfect vision.”
- “Distracting haloes.”
Both reports are accurate. The lens is the same; the eye and the brain are not.
Surgeon’s Note
I have bilateral ZEISS AT LISA tri 839MP trifocal lenses implanted in my own eyes. I made that decision after counselling thousands of patients through the same choice.
I see haloes around headlights at night. I do not consider them distracting. That is my experience, it is not a guarantee of yours, and it is not the basis on which I recommend trifocals to any individual patient. The decision must be made for the eye in front of me.
Plain English
Trifocals give the widest range of vision, but the brain has to learn to interpret split light. Some patients adapt seamlessly. Some notice haloes for months. A small minority do not adapt at all. This cannot be predicted with certainty before surgery.
EDOF Lenses: Smoother Optics, Narrower Range
Extended depth of focus (EDOF) lenses stretch a single focal range rather than splitting light into discrete focal points.⁵ Common platforms include the Tecnis Symfony and the Alcon Vivity.
They are often marketed as “lower halo risk” or “more natural vision.”
The Reality
Some studies do show reduced dysphotopsia compared to trifocals.⁵ This is not the same as saying EDOF lenses do not produce haloes.
In clinical practice, patients with EDOF lenses still report:
- Haloes around point sources of light
- Glare in low light
- Reduced night clarity
And the deeper truth: comparing dysphotopsia between lens platforms across different patients is unreliable. Perception is not purely optical, it is neurological.⁴
Functional Limitation
EDOF lenses provide weaker near vision than trifocals. Most patients still require reading glasses for fine print, prolonged reading, or low light.⁶
Plain English
EDOF lenses often feel more “natural” optically, but they do not eliminate haloes, and they will not eliminate reading glasses.
Monofocal Plus: Incremental, Not Transformational
“Monofocal plus” lenses are enhanced monofocals designed to improve intermediate vision modestly while preserving high contrast sensitivity. Platforms include the Tecnis Eyhance, the Bausch + Lomb LuxSmart, and the RayOne EMV.
They are sometimes positioned as “no haloes” or “the safe premium option.”
The Problem With This Narrative
The claim that monofocal plus lenses do not produce dysphotopsia is misleading. Every optical system interacting with the eye can produce glare, light scatter, and visual disturbance. Perception, again, varies between individuals.
What They Actually Offer
- Excellent distance vision
- Modestly improved intermediate vision
- Minimal improvement in near vision⁷
Plain English
Monofocal plus lenses are a refinement of the standard monofocal. They are not a route to spectacle independence. Patients who want functional vision across all distances will still wear reading glasses with these lenses.
Piggyback IOLs: Not an "Upgrade Strategy"
Piggyback lenses are secondary lenses implanted in addition to an existing IOL. Their primary indications are:
- Correction of residual refractive error after cataract or lens replacement surgery
- Patients unsuitable for laser enhancement⁸
They can also be used to convert a monofocal outcome toward multifocality in selected cases.⁹
The Critical Misconception
Some patients are advised: “Choose a monofocal now, you can always upgrade later.“
This is wrong.
A piggyback solution is not optically equivalent to a primary trifocal implantation. Piggyback configurations involve:
- Inferior optical performance compared to a single, well-positioned trifocal lens
- Increased optical complexity and interface aberrations
- Additional surgical risk
- Limited toric options
Plain English
Piggyback lenses are a correction tool, not a deferred upgrade. If your goal is spectacle independence, plan for it from the outset. The decision is harder later, and the result is usually worse.
Toric Lenses: The Most Underestimated Decision
Astigmatism management is the most consequential, and least understood, part of modern lens surgery. In contemporary practice, more than half of patients require toric correction.¹⁰
What toric lenses do:
- Correct corneal astigmatism at the lens plane
- Improve uncorrected visual acuity
What Patients Are Often Not Told
Toric lenses introduce additional variables:
- Rotation risk: even small misalignment reduces effectiveness substantially¹¹
- May require secondary rotation procedures
- Potential for re-rotation after correction
The Contingency Scenario
If a posterior capsule rupture occurs during surgery, a rare but real event, the planned toric premium lens may not be implantable. The surgical pathway then becomes:
- Three-piece monofocal lens at primary surgery
- Piggyback lens (typically non-toric) at a later date
- Laser enhancement if the eye is suitable
The implication: astigmatism may remain partially uncorrected. This can lead to suboptimal outcomes, patient dissatisfaction, and misattribution to “poor surgery”, when the underlying issue was a rare complication, managed correctly, within a fragmented pathway that left the patient to absorb the cost of every subsequent step.
Plain English
Toric lenses improve vision significantly. They also introduce moving parts. If something unexpected happens during surgery, the plan changes, and what happens next depends entirely on the system around your surgeon.

The System Behind the Surgery Matters More Than the Lens
Lens choice does not exist in isolation. It sits inside a system that must be able to manage:
- Intraoperative complications
- Lens unavailability or change of plan
- Secondary procedures (capsulotomy, rotation, exchange)
- Laser enhancement
- Vitreoretinal support if required
The questions that matter:
- If a complication leads to a lens change, is laser enhancement available, and is it performed by the same surgeon who implanted the lens?
- If the eye needs vitreoretinal support during or after surgery, is that capability in-house, or a referral elsewhere?
- If the visual outcome is not what was discussed at consultation, is enhancement included in the original price, or is it an additional cost?
These are the questions patients rarely ask before booking surgery, and they are the questions that define whether a problem becomes a setback or a crisis. Not all providers operate within systems designed to manage intraocular surgical risk and its downstream consequences. Patients should understand this before proceeding.
Blue Fin Vision® Specifically
Across the Blue Fin Vision® cataract and lens replacement series, dual biometry, in-house vitreoretinal support, fixed enhancement policy with a 24-month window, and named-surgeon continuity from consultation through enhancement are operating standards rather than upgrades.
Six consecutive years of National Ophthalmology Database (NOD) audited outcomes confirm complication rates below national benchmarks across more than 57,000 procedures, with an enhancement rate of approximately 2% under our dual biometry protocol.
The Blue Fin Vision® Advantage exists for the contingency that few clinics discuss openly: what happens when the plan changes.
Haloes, Glare, and the Myth of Predictability
Across every lens type, trifocal, EDOF, monofocal plus, no lens guarantees the absence of haloes or glare.
Perception depends on:
- Neural processing (neuroadaptation)⁴
- Tear film stability¹²
- Corneal aberrations
- Pupil size
- Brain tolerance to optical phenomena
The Honest Position
- Some patients notice haloes with every lens type, including monofocals.
- Some patients notice none, even with trifocals.
- This cannot be predicted with certainty before surgery.
Plain English
Haloes are not a property of the lens alone. They are a property of how your eye and brain interpret light. The lens sets the optics. Your visual system interprets them.
Quick Summary
Trifocal → maximum range, highest independence
EDOF → smoother optics, limited near
Monofocal plus → clarity-first, glasses required
Piggyback → correction only, not upgrade
The lens matters less than how your eye is assessed and how the system manages change.
At a Glance
Lens Type | Range | Summary |
|---|---|---|
Trifocal | Full (distance, intermediate, near) | Lowest glasses dependence; variable halo risk; maximum independence |
EDOF | Distance + intermediate | Moderate glasses dependence; variable halo risk; “natural” optical feel |
Monofocal Plus | Distance + slight intermediate | High glasses dependence; variable halo risk; clarity-focused |
Piggyback | Secondary correction only | Used for residual error correction only |
So Which Lens Should You Choose?
The right lens depends on:
- Your visual priorities
- Your ocular anatomy
- Your tolerance for optical side effects
- Your willingness to adapt
A Simplified Framework
Choose trifocal if:
- You want maximum independence from glasses
- You accept the possibility of haloes
- You understand adaptation may take time
Choose EDOF if:
- You prioritise distance and intermediate vision
- You are comfortable using reading glasses
- You want a potentially smoother visual experience (not guaranteed)
Choose monofocal plus if:
- You prioritise clarity and contrast
- You are comfortable wearing glasses for near and intermediate tasks
- You want minimal optical complexity
Consider piggyback only if:
- You have residual error after surgery
- You are not suitable for laser correction
The Most Important Question Isn't the Lens
Patients ask: “Which lens is best?”
The question “which lens is best” is clinically meaningless.
The better question: “How is the decision made for my eyes?”
Because biometry accuracy, tear film optimisation, macular assessment, and surgical planning matter more than the label on the lens.¹³ A trifocal in an eye with untreated dry eye, an unrecognised epiretinal membrane, or inaccurate biometry will not deliver what the brochure promised.
The lens is the final variable. The eye is the first one.

How to Choose the Right Lens and the Right Surgeon
Understanding lens types is only part of the decision.
The outcome depends on how that decision is made.
When comparing providers, patients should ask:
How Is My Eye Being Assessed?
- Is tear film optimised before biometry?
- Is macular OCT performed routinely?
- Are higher-order aberrations considered?
How Is the Lens Decision Made?
- Is it based on lifestyle and ocular anatomy?
- Or is it based on a standardised “lens tier” approach?
What Happens if the Plan Changes?
- If a complication occurs, what is the pathway?
- Is vitreoretinal support available immediately?
- Is enhancement included, or additional?
Who Manages the Full Journey?
- Is the same surgeon responsible for consultation, surgery, and enhancement?
- Or is care fragmented across providers?
The most important decision is not the lens.
It is choosing a system that understands how to select, deliver, and adapt that lens to your eye.
Final Thought
Two patients. Same lens. Different experience.
Not because one lens was better.
Because biology varies. Perception varies. Planning varies.
Clinical Takeaway
The lens you choose will not, on its own, determine your visual outcome.
Biometry, ocular surface, macular health, surgical execution, and the system that surrounds the surgery matter more than the optical category on your consent form.
There is no perfect lens. There is only the right lens for the right eye, chosen within the right system.
The lens is chosen in minutes. The outcome is lived with for decades.
Decide on the lens last, after the eye has been understood first.
-Mr Mfazo Hove, Consultant Ophthalmic Surgeon
The wrong lens is rarely the result of a bad operation. It is almost always the result of a poor decision process.
References
- de Vries NE, Webers CA, Touwslager WR, Bauer NJ, de Brabander J, Berendschot TT, Nuijts RM. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859-865.
- Cochener B, Boutillier G, Lamard M, Auberger-Zagnoli C. A comparative evaluation of a new generation of diffractive trifocal and extended depth of focus intraocular lenses. J Refract Surg. 2018;34(3):158-167.
- Pedrotti E, Carones F, Aiello F, Mastropasqua R, Marchini G. Comparative analysis of visual outcomes with 4 intraocular lenses: monofocal, multifocal, and extended range of vision. J Cataract Refract Surg. 2018;44(2):156-161.
- Rosa AM, Miranda AC, Patricio MM, McAlinden C, Silva FL, Castelo-Branco M, Murta JN. Functional magnetic resonance imaging to assess neuroadaptation to multifocal intraocular lenses. J Cataract Refract Surg. 2017;43(10):1287-1296.
- Cochener B, Concerto Study Group. Clinical outcomes of a new extended range of vision intraocular lens: International Multicenter Concerto Study. J Cataract Refract Surg. 2016;42(9):1268-1275.
- Monaco G, Gari M, Di Censo F, Poscia A, Ruggi G, Scialdone A. Visual performance after bilateral implantation of 2 new presbyopia-correcting intraocular lenses: trifocal versus extended range of vision. J Cataract Refract Surg. 2017;43(6):737-747.
- Mencucci R, Favuzza E, Caporossi O, Savastano A, Rizzo S. Comparative analysis of visual outcomes, reading skills, contrast sensitivity, and patient satisfaction with two models of trifocal diffractive intraocular lenses and an extended range of vision intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2018;256(10):1913-1922.
- Gayton JL, Sanders VN, Van der Karr M, Raanan MG. Piggybacking intraocular implants to correct pseudophakic refractive error. J Cataract Refract Surg. 2000;26(10):1519-1522.
- Hsuan JD, Caesar RH, Rosen PH, Rosen ES, Gore CL. Correction of pseudophakic anisometropia with the STAAR Collamer implantable contact lens. J Cataract Refract Surg. 2002;28(1):44-49.
- Hoffmann PC, Hütz WW. Analysis of biometry and prevalence data for corneal astigmatism in 23,239 eyes. J Cataract Refract Surg. 2010;36(9):1479-1485.
- Novis C. Astigmatism and toric intraocular lenses. Curr Opin Ophthalmol. 2000;11(1):47-50.
- Epitropoulos AT, Matossian C, Berdy GJ, Malhotra RP, Potvin R. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41(8):1672-1677.
- Norrby S. Sources of error in intraocular lens power calculation. J Cataract Refract Surg. 2008;34(3):368-376.
ABOUT THE AUTHOR
Mr Mfazo Hove
Consultant Ophthalmic Surgeon
MBChB MD FRCOphth CertLRS
Mr Mfazo Hove is a Consultant Ophthalmic Surgeon with experience spanning more than 57,000 procedures. He completed 6.5 years of specialist training at Moorfields Eye Hospital and served for five years as a consultant at the Western Eye Hospital, Imperial College Healthcare NHS Trust. He is the founder of Blue Fin Vision®, a consultant-led private ophthalmology practice operating across London, Essex, and Hertfordshire. His clinical expertise encompasses advanced cataract surgery, refractive lens replacement, laser vision correction, and implantable Collamer lenses (ICL).
A ZEISS Key Opinion Leader, Mr Hove is a respected international speaker with five invited engagements across seven cities in 2026:
- ZEISS China tour (Changsha, Shanghai, and Hangzhou, April – ZEISS APAC User Meeting)
- RCOphth Annual Congress – May – Manchester
- ZEISS EMEA User Meeting (Istanbul)
- ZEISS Lausanne User Meeting (Lausanne)
- European Society of Cataract and Refractive Surgeons Annual Congress (ESCRS, London)
Related Topics
Start Here: The Full Decision Framework
Choosing the Right Lens for You
Astigmatism, Biometry and Lens Performance
Haloes, Glare and Adaptation After Surgery
Long-Term Outcomes
Schedule Your Consultation Today
If you are considering cataract surgery or refractive lens exchange and want a consultant-led assessment that begins with the eye, not the lens catalogue, the Blue Fin Vision® team would be glad to discuss your options. Consultations are available across our London, Hertfordshire, and Essex locations, including Harley Street, Weymouth Street, Hatfield, Chelmsford, and Chase Lodge Hospital. Please contact the team to book a consultation.


