
China Is Solving Presbyopia at Scale – The Rest of Us Are Not Ready
- Posted
- Medically Reviewed by: Mr Mfazo Hove, Consultant Ophthalmic Surgeon
- Author: Chris Dunnington
- Published: April 20, 2026
- Last Updated: May 1, 2026
390 Million Patients, Three Cities, Five Venues. Invited UK Faculty at the “Bridging Horizons, Converging Minds” UK-China Summit on Presbyopia Correction & HORIZON 2026 ZEISS APAC Ophthalmology Symposium, Shanghai, 17-19 April 2026
China does not need to learn how to perform presbyopia surgery.
It is now solving how to deliver it at scale.
That is why I was invited.
In China, 390 million adults aged 35 and over have presbyopia. Prevalence in the 52-and-over cohort is near-universal. Nearly 70% are untreated.⁸ That is the patient base Chinese ophthalmology leadership is now mobilising to address, at a scale that dwarfs any Western market.
In April 2026, I was selected as invited UK faculty at the “Bridging Horizons, Converging Minds” UK-China Summit on Presbyopia Correction, held at Shanghai Aier Eye Hospital Academic Centre on 19 April 2026, and as international faculty at the HORIZON 2026 ZEISS APAC Ophthalmology Symposium across 17-19 April. A three-city tour across Changsha, Shanghai, and Hangzhou followed. The invitation was not to teach surgery. Chinese refractive surgeons can operate. It was to help design the decision frameworks, consultation pathways, and system-level protocols that allow Western-standard presbyopia outcomes to be delivered at the highest patient volumes in the world.
What is happening in China will define how presbyopia correction is delivered globally over the next decade. Every major healthcare system, including the NHS, US Medicare, and EU national frameworks, is moving toward a future of fewer refractive surgeons per capita, thinner optometric support, and rising patient expectations for premium outcomes. China is already operating inside that future. That is why the frameworks built on this tour matter far beyond China.

ZEISS Certificate of Appreciation, Faculty Member, HORIZON 2026 ZEISS APAC Ophthalmology Symposium, Shanghai, 17-19 April 2026. Signed by Manoj Venkiteshwar, Global Head of Medical Affairs, ZEISS.
I am a consultant ophthalmic surgeon whose practice integrates both laser and lens-based presbyopia correction within a single clinical pathway, an overlap that remains uncommon globally, particularly within a consultant-led private practice.
As a surgeon, as a patient, and as a practice owner, using ZEISS is the first decision I make.

Presenting at the Bridging Horizons, Converging Minds UK-China Summit, Shanghai Aier Eye Hospital Academic Centre, 19 April 2026. Behind: the “I do” video testimonial, surgeon, patient, and practice owner framing, with the ZEISS AT LISA tri trifocal IOL.
What I Was Asked to Deliver in China
The Chinese centres did not ask for surgical training. They asked for system architecture. The specific deliverables were:
- Decision frameworks for laser-versus-lens presbyopia correction at volume.
- Protocolised triage for the patient whose result falls short of expectation.
- Ordered management of the unhappy patient under team-based follow-up.
- Pre-consented enhancement pathways for residual refractive error.
- Framework-led lens selection executable by a consistent team.
- Pre-consultation architecture that moves consent upstream of the clinical slot.
Each of these is a systems problem, not a surgical problem. Surgery in a Chinese tier-1 refractive centre is performed at an exceptional standard. The question Chinese ophthalmology leadership is now working through is how to wrap that surgical capability inside consultation, triage, consent, and follow-up architecture that reproduces Western refractive outcomes at Chinese throughput. That is the work I was deployed to do.
Four Structural Asymmetries Driving the Redesign
The UK model cannot be copied into China. It cannot be copied because it was designed for a delivery envelope China does not have. Four structural asymmetries force the redesign.
One. Patient density. A 2024 national survey counted 48,652 ophthalmologists across mainland China, 1.7 per 57,000 population, meeting the WHO Vision 2020 benchmark at aggregate.¹ But the mean patient-to-ophthalmologist ratio is 2,585 to 1, and in Shanghai and Zhejiang, both regions I visited, it exceeds 4,000 to 1.¹ The equivalent UK ratio is a small fraction of that.²
Two. Surgical sub-population. Roughly one in three Chinese ophthalmologists performs cataract surgery independently, and the cohort trained in modern phacoemulsification, premium IOL work, and corneal laser refractive surgery is a fraction of that again. The density of surgeons capable of trifocal implantation and presbyopia laser correction is concentrated in a small number of urban tertiary centres.
Three. Thin optometric support. The same 2024 survey reported 0.47 optometrists per 57,000 population, well below the global average.¹ In the UK, preoperative assessment, patient education, and postoperative refractive management are routinely distributed across optometrists and allied staff. In China, that support layer is far thinner. More cognitive load falls on the surgeon at the point of consultation, and the consultation is already compressed.
Four. Demand is already here. The 2023 China Presbyopia Population Insight Report documents 390 million Chinese adults aged 35 and over with presbyopia, a 56.9% prevalence rate, near-universal prevalence in the 52-plus cohort, and approximately 70% of affected patients currently untreated.⁸ The capacity gap is not theoretical. It is the largest untreated refractive patient base in modern healthcare, and the policy driver behind every venue I spoke at.
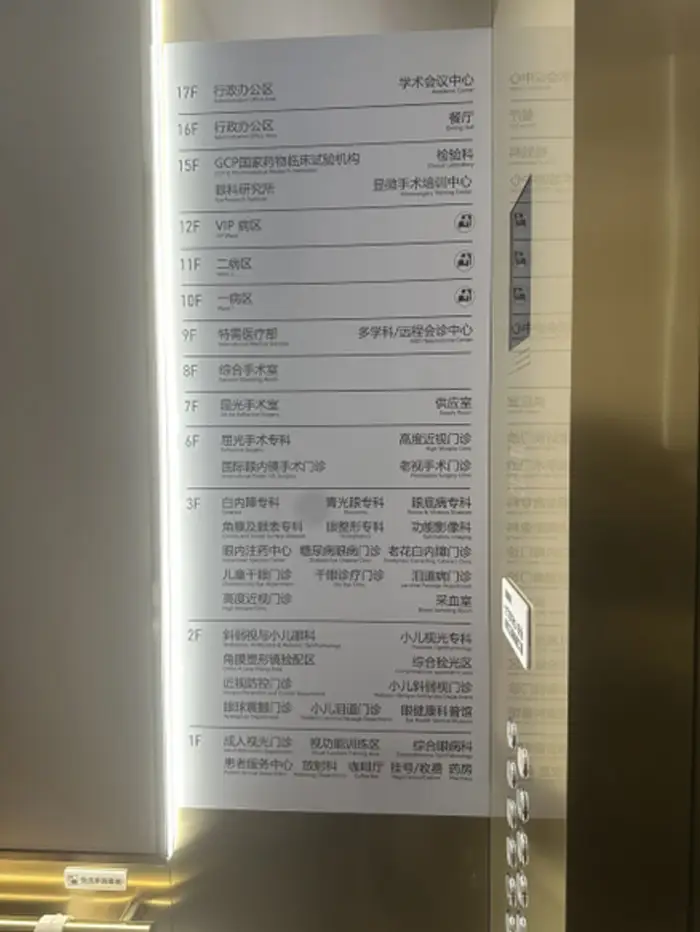
Clinical directory at one of the Chinese tertiary eye centres visited, a dedicated Presbyopia Surgery Clinic, International Phakic IOL Surgery Clinic, Presbyopic Correcting Cataract Clinic, Refractive Surgery Theatre, and Microsurgery Training Centre. Sub-specialty sophistication is high; distribution is concentrated.
The UK consultation could not be imported because it was designed for a ratio of patient demand to consultant supply that no longer exists anywhere, and that will not exist in the UK either within a decade. China is the forward-looking test case, not the exception.
The Frameworks I Translated
Across every centre, the substance of the exchange was the same. We walked through what we do in the UK, component by component, and worked out which elements translate directly, which need adaptation, and which cannot move across at all. Five translation points did most of the work.
- Consultation time
UK private refractive consultation slot: 30 to 45 minutes of consultant time, often preceded by a separate optometrist assessment, governed by NICE guidance on cataract and refractive management.³ Chinese tier-1 refractive consultation: a small fraction of that. The Montgomery-standard conversation, including realistic expectations, dysphotopsia, and residual refractive error probability, does not compress into five minutes. It has to be distributed upstream through standardised pre-consultation video education, structured biometry protocols, and patient-facing literature that does the explanatory work before the patient sits in front of the surgeon. Consent becomes a pathway, not a conversation. The clinical standard stays the same. The delivery model changes.
- Lens selection logic
In a UK private practice, lens selection is an individualised, case-by-case conversation with the consultant over two or more preoperative visits, informed by published comparative data on multifocal, trifocal, and extended-depth-of-focus platforms.⁴ ⁵ At Chinese throughput, selection has to be framework-led. The inputs do not change: age, refractive error, corneal topography, lens status, ocular surface, pupil behaviour, night-driving requirements, tolerance for photic phenomena, functional vision priorities. What changes is how that logic is documented, sequenced, and applied. It has to be auditable, teachable, and executable by a consistent team, not a single consultant’s private judgement.
- Laser versus lens decision
This is the decision most Chinese centres wanted explicit guidance on, because most of their refractive surgeons operate one platform rather than both. The framework does not change under volume.⁶ The decision is driven by the eye, not by the surgeon’s preferred tool. The operational adaptation is that the referral pathway between laser and lens surgery has to be pre-built, not improvised. In a centre where different surgeons run different platforms, pointing the patient to the correct operation requires protocolised triage, not collegial judgement at the point of consultation.
- The unhappy patient
This is the hardest question in presbyopia surgery and the one most under-discussed at congress level. The framework is ordered. Rule out residual refractive error first. Rule out posterior capsule opacification second. Rule out ocular surface disease third. Only then open the neural adaptation conversation. Lens explant is the last door, not the first. The adaptation for Chinese practice is that the patient who is unhappy at follow-up may not be seen by the operating surgeon, as post-operative review is frequently team-based. That means the triage algorithm has to be explicit and documented, so that whoever sees the patient catches the reversible causes before the patient decides they have been failed.
- Residual refractive error management
Every premium lens patient needs a defined pathway for laser enhancement if biometry does not land where it should, and that pathway must be disclosed before the first operation, not after. The published risk factors for post-cataract refractive error are well-characterised and should inform biometry protocol design.⁷ In the UK, enhancement is usually same-consultant, same-week, same-site. In Chinese practice, enhancement may require a different surgeon, different platform, different facility. The patient must consent to the whole pathway up front, or the conversation after a missed target becomes one about complaint rather than about care.
The Chinese surgeons in the room were not asking to be taught. They were problem-solving, pressure-testing UK frameworks against their operational reality and flagging which elements would break under 60-plus consultations per day. The refinements were bidirectional. Several of the adaptations we worked through are genuine improvements on how we do things in London.
The Blue Fin Vision® Doctrine at Chinese Scale
The frameworks I brought to China are not improvisations. They sit inside the Blue Fin Vision® Doctrine, a nine-pillar institutional philosophy anchored to a single principle: to achieve the immeasurable, you must measure everything.
The doctrine states that refractive outcomes at scale are not a function of individual surgical brilliance. They are a function of measured systems, structured pathways, and documented decisions that survive the absence of any single consultant. What imports into Chinese tier-1 centres is not UK seniority or UK training. It is the doctrinal commitment to systems over individuals, measured outcomes over reputations, and structured pathways over ad-hoc clinical judgement.
The Blue Fin Vision® Advantage, four consecutive years of published National Ophthalmology Database (NOD) outcomes, a posterior capsule rupture rate of approximately 0.2% against a national benchmark of ~0.79%, and named surgeon transparency across every case, is the evidence base that a systems-first approach to refractive surgery produces measurably better outcomes than surgeon-first approaches. It is also the reason the invitation came. Data travels. Frameworks that generate measurable outcomes travel faster.
What Actually Happened on the Ground
Three working days. Three cities. Five venues. Each stop carried its own clinical register and its own audience, but every stop tested the same thesis: Western refractive frameworks can translate into Chinese ophthalmology, if they are rebuilt for Chinese throughput. What follows is not a programme report. It is what actually happened at each venue, and what each venue surfaced that could not be extracted any other way.
HORIZON 2026 ZEISS APAC Ophthalmology Symposium (Shanghai, 17-19 April 2026)
The anchor event of the programme. HORIZON 2026 convened the ZEISS regional faculty across Asia-Pacific under the theme “New Trends in Digitally-Driven Refractive Cataract and Presbyopia.” Chairs were Prof Xingchao Shentu and Prof Tao Guo. Co-faculty included Prof Yi Lu, Dr Rosman Mohamad, Dr Harsha Nagaraj, Prof Guangying Zheng, Prof Hao Cheng, and Prof Jianyu Yang. The audience spanned hundreds of attending ophthalmologists in the hall, with extended livestream distribution across the Chinese ophthalmology community.
My presentation covered trifocal IOL outcomes, integration of the ZEISS AT LISA tri 839MP platform into a UK consultant-led practice, and system-based delivery of ophthalmic care, the methodology underpinning Blue Fin Vision®’s four consecutive years of published National Ophthalmology Database (NOD) outcomes, including a posterior capsule rupture rate of approximately 0.2% against a national benchmark of ~0.79%. The “I do” video testimonial, framing the ZEISS decision from three positions simultaneously: surgeon, patient, practice owner, drew specific Q&A engagement, because it answered what Chinese delegates were actively weighing: what does commitment to a single premium platform look like across a career?
Two KOL-to-KOL expert interviews were also recorded inside the HORIZON 2026 programme as part of the faculty remit. At the close of the symposium, ZEISS issued a Certificate of Appreciation signed by Manoj Venkiteshwar, Global Head of Medical Affairs, documentary confirmation of faculty status across the three days.

HORIZON 2026 ZEISS APAC Ophthalmology Symposium, Faculty panel for the session on New Trends in Digitally-Driven Refractive Cataract and Presbyopia, Shanghai, April 2026.
Bridging Horizons, Converging Minds UK-China Summit on Presbyopia Correction (Shanghai Aier Eye Hospital Academic Centre, 17F, 19 April 2026)
A bilateral summit convened expressly to upgrade China’s clinical pathway for presbyopia correction, co-chaired by Dr Li Yong, Deputy Director of Shanghai Aier Eye Hospital, alongside senior Chinese faculty from refractive surgery, cataract, retina, glaucoma, and cornea subspecialties. The summit focused on four core themes: overseas standardised presbyopia correction workflows, multidisciplinary (MDT) care models, individualised surgical selection for the presbyopic patient, and full-lifecycle visual management.
I was invited as UK faculty to bring the Western consultant-led decision framework into direct comparison with the Chinese tier-1 delivery model. The discussion was not one-directional. Chinese delegates interrogated how the UK consultation protocol would survive a 4,000-to-1 patient-to-ophthalmologist ratio, how the Montgomery consent standard would translate into a compressed clinical slot, and how enhancement pathways should be consented across different surgeons and different platforms. Every element of the UK framework was stress-tested against Chinese operational reality in real time. Several of the adaptations that emerged are now genuine improvements on UK practice.
The summit was framed by Chinese media coverage (see below) as marking Shanghai Aier’s formal transition into a multidisciplinary, one-stop, full-lifecycle presbyopia care model, with international expert dialogue identified as the mechanism for that upgrade.

UK and Chinese faculty at the Bridging Horizons, Converging Minds UK-China Summit on Presbyopia Correction. Shanghai Aier Eye Hospital Academic Centre, 19 April 2026.
Aier Eye Hospital, Changsha
Aier Group’s flagship presbyopia and refractive centre in Hunan province, and the venue for the opening lecture of the tour. The session covered presbyopia correction strategy, trifocal intraocular lens selection logic, and full-arc management of the modern presbyopic patient from first consultation through long-term follow-up. The audience comprised refractive and cataract surgeons from across the Aier Changsha network.
The Q&A focused disproportionately on the unhappy patient, how the UK framework orders the differential between residual refractive error, posterior capsule opacification, ocular surface disease, and neural adaptation; and how that ordered triage is documented so that any team member catches reversible causes before the patient reaches the explant conversation. This is the question most under-discussed at congress level in China, and the one that carried most weight at this venue.
Shanghai New Vision Eye Hospital
A clinical exchange and lecture focused on pathway design: the architecture of the consultation itself, and how Montgomery-standard consent can be distributed upstream through structured pre-consultation education, standardised biometry protocols, and patient-facing literature when consultant time at the point of care is compressed. The residual refractive error discussion centred on the design of pre-consented enhancement pathways for premium lens patients, disclosed before the first operation, not negotiated after a missed target.
Hangzhou Chaoju Eye Hospital
Hangzhou Chaoju Eye Care (朝聚眼科) treated the visit as an institutional event. A full-height cascading rose wall, five metres tall, flanked the main entrance. A branded welcome was projected across the hospital window: “Welcome Mr Mfazo Hove (Substantive Consultant Ophthalmologist, Western Eye Hospital, Imperial College Healthcare) to our hospital.” An interior welcome easel stood in the main foyer. The senior clinical team assembled outside to receive me on arrival. This is not polite hospitality. It is how a Chinese tier-1 private eye hospital signals the institutional weight it attaches to a visiting international faculty member, and how seriously it takes the content of the exchange that is about to follow.

Welcome at Hangzhou Chaoju Eye Care (朝聚眼科), a cascading rose wall and projected welcome signage on the storefront window, April 2026.
The clinical content matched the register of the welcome. The session was a systems and workflow leadership discussion in Zhejiang province, a region where the patient-to-ophthalmologist ratio exceeds 4,000 to 1. The brief was explicit: how to scale premium refractive care at the top end of Chinese volume without compromising consultation quality. The discussion centred on framework-led lens selection (auditable, teachable, executable by a consistent team), protocolised triage between laser and lens platforms where different surgeons operate different modalities, and team-based follow-up architecture for the premium refractive patient.

With the senior clinical team at Hangzhou Chaoju Eye Care, April 2026.

Interior welcome easel, Hangzhou Chaoju Eye Care.
Across every venue, the delivery footprint was larger than the room. Each stop combined an in-person audience of hundreds of attending ophthalmologists with extended online livestream distribution across the Chinese ophthalmology community, turning a three-day tour into a national-scale teaching intervention.
Four Observations That Surprised Me in China
Four things about Chinese refractive ophthalmology genuinely surprised me, things I did not expect from the outside and will not forget from the inside.
- Subspecialty sophistication rivals London and New York.
The tier-1 Chinese eye hospital is not a translation of a Western cataract centre. It is its own institution, with dedicated clinics for Presbyopia Surgery, International Phakic IOL Surgery, Presbyopic Correcting Cataract, High Myopia, Dry Eye, Oculoplastics, Ocular Surface, Lacrimal, Glaucoma, and Paediatric Ophthalmology, all on separate floors of the same building, with a dedicated Microsurgery Training Centre above and a Clinical Laboratory and Eye Research Institute above that. What is concentrated in China is access, not capability.
- The willingness to interrogate, not absorb.
I had expected polite deference to UK framework content. I encountered the opposite. Chinese senior surgeons pressure-tested every element of the UK consultation, consent, and follow-up pathway against their operational envelope and flagged specifically which parts would break and why. That is the posture of a system confident enough to adopt selectively, not copy wholesale. It is also the posture of a system that will overtake.
- National media velocity.
The Bridging Horizons summit was carried on five Chinese national platforms within hours. A comparable UK clinical summit reaches trade press in two weeks. The signal is not just that Chinese media covers ophthalmology. It is that Chinese ophthalmology leadership treats clinical pathway upgrades as national news. Healthcare policy positioning in China moves at a speed the UK is not prepared for.
- The personal volume.
Chinese refractive surgeons are running 60 to 100 presbyopic consultations per day. That number, repeated across multiple venues by people sleeping less than I do, is the most important statistic of the tour. It is not sustainable individually. It is exactly why the systems work is urgent, in China today, and in every Western system within a decade.
KOL-to-KOL Evidence Captured Inside ZEISS APAC
Two interviews were captured inside the HORIZON 2026 programme as part of the faculty remit. These are not patient outcome reports. They are not peer-reviewed endpoints. They are the private clinical decisions of senior ophthalmologists, the register of evidence that shapes platform confidence across a surgical career, and that almost never reaches the public literature. Access to this class of evidence is a feature of platform-level engagement, not speaker-level engagement. It is what the HORIZON 2026 programme is built to generate.
Dr Claudia Naval, ZEISS AT ELANA Trifocal, Implanted by His Ophthalmologist Daughter
A practising ophthalmologist receiving a trifocal IOL from his own daughter is one of the strongest real-world validations of a lens platform.
Picture the moment.
A senior ophthalmologist, decades of accumulated clinical judgement, every premium intraocular lens platform evaluated and catalogued, every compromise identified, every risk counselled to patients, agrees to let his own daughter, herself an ophthalmologist, implant a trifocal intraocular lens into his eye. Every competing platform he has assessed across a career converges into a single decision on a single morning, made inside his own family.
He chose the ZEISS AT ELANA trifocal.
That is a quiet decision. It is also the highest-trust endorsement a premium intraocular lens platform can receive in global ophthalmology. Surgeon endorsements at congress are cheap. Industry honoraria buy lectures. What cannot be bought, and cannot be manufactured at any price, is the decision a senior surgeon makes when he lets his own child perform the operation, when he bets his own uncorrected visual future on the optical design his daughter will be clinically accountable for.
The ZEISS platform passed that test. Dr Naval gave the interview on the record inside the HORIZON 2026 programme. He did so because he considers the decision worth documenting. So do I.
A Leading International Presbyopia Pathways Specialist
The second interview examined the structural differences between how presbyopia correction is offered in North America, Europe, and Asia, and where clinical decision-making converges despite those differences. The consensus: the clinical gap between regions is narrower than it used to be. The divergence is in how each region handles scale.
Chinese National Media Coverage of the Summit
The Bridging Horizons, Converging Minds UK-China Summit was covered across major Chinese national news distribution platforms within hours of the event, signalling the weight Chinese ophthalmology leadership attached to the exchange. The summit and my role in it were syndicated through:
- Sina News (新浪), one of China’s largest general-news portals.
- NetEase News (网易 / Wangyi), major national media group.
- Weibo (微博), China’s dominant public social platform.
- China.com (中華網), state-affiliated national news portal.
- Caixun (财讯网), financial and health news vertical.
Chinese media coverage framed the summit as marking Shanghai Aier Eye Hospital’s formal transition into a multidisciplinary, one-stop, full-lifecycle presbyopia care model, with international expert dialogue identified as the mechanism for that upgrade. The strategic positioning in Chinese national media is unambiguous: international expertise, including mine, is now part of the institutional narrative of China’s presbyopia correction era.
Where the Real Conversations Happened
The Shanghai 1930s Ball was black tie. The karaoke rooms that followed were not. Both were where the actual questions came out.
Over dinner, and across the microphone, Chinese surgeons, some of whom had presented on the symposium platform that afternoon with perfect composure, admitted what they struggle with. The patient who is unhappy after a technically perfect trifocal implant. The 70-year-old who expected reading vision that matches her 40-year-old self. The private decision calculus when a patient with borderline topography still wants LASIK. The fear of the explant conversation. The moment when team-based follow-up means the unhappy patient sits in front of a colleague who did not operate.
These are the questions that do not get asked from a lecture-hall floor. They only come out when the cameras are off and the microphone has been handed to someone attempting Frank Sinatra. They are also the questions that matter most, the ones that drive the design of the next generation of presbyopia decision frameworks. Chinese and UK faculty, across a language barrier, often with a single delegate’s English sharpening by the hour, worked through them around dinner tables, in hotel bars, and in taxi queues late into the Shanghai night.
If you were in the room, you heard them. If you were not, no conference report will ever capture them. That is the point of being invited in the first place.

HORIZON 2026 ZEISS APAC Ophthalmology Symposium, Shanghai, April 2026.
Why the UK Model Breaks Under Pressure
The UK is not structurally different from China. It is earlier on the same curve.
Every structural pressure driving Chinese ophthalmology toward systems-based delivery is already present in UK private refractive practice, just less advanced. The consultation structures we have built our careers inside are not stable. They are a luxury of current supply-demand economics that will not survive the decade.
- Ophthalmologist supply is flattening. Consultant training numbers are not expanding at the rate of population ageing. Private consultant capacity is plateauing as the NHS training pipeline narrows.
- Patient demand is rising. The UK 50-plus cohort is the largest it has ever been, with the highest disposable income in modern history, and the highest expectations of premium refractive outcomes.
- Consultation time is already under pressure. The 30-to-45-minute UK private refractive slot is not a stable equilibrium. It is the first thing the capacity squeeze takes.
- Montgomery consent is not going anywhere. The legal standard will not compress just because the clinical slot does. Surgeons who do not redesign pre-consultation architecture now will be caught between an inflexible legal standard and an increasingly compressed clinical slot, and the collision will be measured in complaints before it is measured in outcomes.
- Patients already compare across borders. The patient who has researched Chinese and US premium IOL platforms before arriving in a London consulting room is the new norm, not the outlier. Surgeons who cannot articulate their system, their outcomes, their protocol, and their enhancement pathway in plain language will lose those patients.
Here is the statement that matters. Refractive surgery is no longer a surgical discipline. It is a systems discipline. Surgeons who do not build pathways will not survive the next decade. The surgeons, clinical groups, and platforms that build the better systems will define it.
China is not a warning. China is a preview.
The Thesis
The frameworks I translated in Shanghai, Changsha, and Hangzhou are not China-specific. They are system-agnostic. They describe how to deliver Western-standard refractive outcomes inside a constrained delivery envelope, in Chinese tertiary centres now, and in UK private, NHS, and European practice as that envelope tightens.
The 2026 ZEISS faculty year continues into the EMEA Symposium in Istanbul, the Lausanne programme, and ESCRS London. Each venue carries the same clinical thesis, calibrated for the local delivery envelope. The China tour was the opening block. It was not a standalone event.
The future of ophthalmology will not be decided by who operates best. It will be decided by who builds systems that allow average surgeons to deliver exceptional outcomes consistently.
That is the shift. Individual surgical brilliance, uncompressed consultation time, single-consultant follow-up: these are luxuries of a previous era. The era now beginning is defined by measured outcomes, structured pathways, protocolised decision frameworks, and team-based delivery. The surgeons, clinical groups, and platforms that build those systems will define the decade. Those that cling to the surgeon-first model will watch their patients choose otherwise.
This is the thesis Blue Fin Vision® was built around. It is the thesis the Blue Fin Vision® Doctrine codifies. It is the thesis the China tour confirmed. And it is the thesis that will carry across the remainder of the 2026 ZEISS international faculty year, and the decade beyond it.
Clinical Takeaway
Systems Over Individuals. Measured Outcomes Over Reputations. Structured Pathways Over Judgement.
These are the three commitments the Blue Fin Vision® Doctrine carries into any healthcare system, and they are what Chinese ophthalmology invited me to translate for its refractive surgery future. The UK will face the same structural pressures inside a decade. The frameworks built in Shanghai, Changsha, and Hangzhou are not just for China. They are the architecture of how premium refractive surgery gets delivered everywhere, as the global supply of refractive surgeons flattens against rising global demand.
The future of ophthalmology will not be decided in the operating theatre.
It will be decided in the pathway.
References
- Wang JD, Chen CX, Liu MR, Guo DD, Wang HY, Li YY, Zhou Q, Jonas JB, Wang NL. National-wide survey of ophthalmic human resources in China in 2021. BMC Health Services Research. 2024;24:1490.
- Resnikoff S, Lansingh VC, Washburn L, Felch W, Gauthier TM, Taylor HR, Eckert K, Parke D, Wiedemann P. Estimated number of ophthalmologists worldwide (International Council of Ophthalmology update): will we meet the needs? British Journal of Ophthalmology. 2020;104(4):588-592.
- National Institute for Health and Care Excellence. Cataracts in adults: management (NG77). London: NICE; 2017.
- Cochener B, Boutillier G, Lamard M, Auberger-Zagnoli C. Visual and refractive outcomes after implantation of a fully diffractive trifocal lens. Journal of Cataract and Refractive Surgery. 2012;38(12):2060-2067.
- Pedrotti E, Carones F, Aiello F, Mastropasqua R, Marchini G. Comparative analysis of visual outcomes with multifocal intraocular lenses. American Journal of Ophthalmology. 2018;190:61-69.
- Kohnen T, Breyer D, Klaproth OK. Presbyopia correction in modern cataract surgery. Eye. 2017;31(2):163-170.
- Lundström M, Dickman M, Henry Y, Manning S, Rosen P, Tassignon MJ. Risk factors for refractive error after cataract surgery: analysis of 282,811 cases. Journal of Cataract and Refractive Surgery. 2018;44(4):447-452.
- 2023 China Presbyopia Population Insight Report (《2023中国老花眼人群洞察报告》). Cited in: “Bridging Horizons, Converging Minds” Shanghai Aier UK-China Summit on Presbyopia Correction press materials, Shanghai Aier Eye Hospital, 19 April 2026.
ABOUT THE AUTHOR
Mr Mfazo Hove
Consultant Ophthalmic Surgeon
MBChB MD FRCOphth CertLRS
Mr Mfazo Hove is a Consultant Ophthalmic Surgeon with experience spanning more than 57,000 procedures. He completed 6.5 years of specialist training at Moorfields Eye Hospital and served for five years as a consultant at the Western Eye Hospital, Imperial College Healthcare NHS Trust. He is the founder of Blue Fin Vision®, a consultant-led private ophthalmology practice operating across London, Essex, and Hertfordshire. His clinical expertise encompasses advanced cataract surgery, refractive lens replacement, laser vision correction, and implantable Collamer lenses (ICL).
A ZEISS Key Opinion Leader, Mr Hove is a respected international speaker with five invited engagements across seven cities in 2026:
- ZEISS China tour (Changsha, Shanghai, and Hangzhou, April – ZEISS APAC User Meeting)
- RCOphth Annual Congress – May – Manchester
- ZEISS EMEA User Meeting (Istanbul)
- ZEISS Lausanne User Meeting (Lausanne)
- European Society of Cataract and Refractive Surgeons Annual Congress (ESCRS, London)


